
DOP13 Clinical and endoscopic response to ustekinumab in Crohn’s disease: Week 16 interim analysis of the STARDUST trial
S. Danese1, S. Vermeire2, G. D’Haens3, J. Panés4, A. Dignass5, F. Magro6, M. Nazar7, M. Le Bars8, S. Sloan9, M. Lahaye10, L. Ni11, M. Daperno12, M. Lukáš13, A. Armuzzi14, M. Löwenberg3, D.R. Gaya15, L. Peyrin-Biroulet16
1Humanitas University, Department of Gastroenterology, Milan, Italy, 2University Hospitals Leuven, Department of Gastroenterology, Leuven, Belgium, 3University of Amsterdam, Academic Medical Centre, Amsterdam, The Netherlands, 4Hospital Clinic of Barcelona CIBERehd, Department of Gastroenterology, Barcelona, Spain, 5Agaplesion Markus Hospital, Department of Medicine I, Frankfurt/Main, Germany, 6Department of Pharmacology and Therapeutics, Institute for Molecular and Cell Biology, Faculty of Medicine, University of Porto, and Department of Gastroenterology, Hospital de Sao Joao, Porto, Portugal, 7Janssen-Cilag Polska Sp. z o.o, Medical Affairs, Warsaw, Poland, 8Janssen-Cilag, Medical Affairs, Issy-les-Moulineaux, France, 9Janssen Global Services LLC, Medical Affairs, Horsham, PA, USA, 10Janssen-Cilag B.V., Medical Affairs, Breda, The Netherlands, 11Janssen-Cilag Russia, Medical Affairs, Moscow, Russian Federation, 12Mauriziano Hospital, Gastroenterology Unit, Turin, Italy, 13Clinical Center ISCARE, Clinical and Research Center for Inflammatory Bowel Diseases, Prague, Czech Republic, 14Fondazione Policlinico Universitario A. Gemelli IRCCS Università Cattolica del Sacro Cuore, IBD Unit Presidio Columbus, Rome, Italy, 15Glasgow Royal Infirmary, Department of Gastroenterology, Glasgow, UK, 16University Hospital of Nancy University of Lorraine, INSERM Unité 954 and Department of Hepato-Gastroenterology, Houdemont, France
Background
Treat-to-target (T2T) strategy may optimise IBD disease management. We describe interim clinical and endoscopic results of the STARDUST trial in Crohn’s disease (CD) patients, following 16 weeks (W) of ustekinumab (UST) induction.
Methods
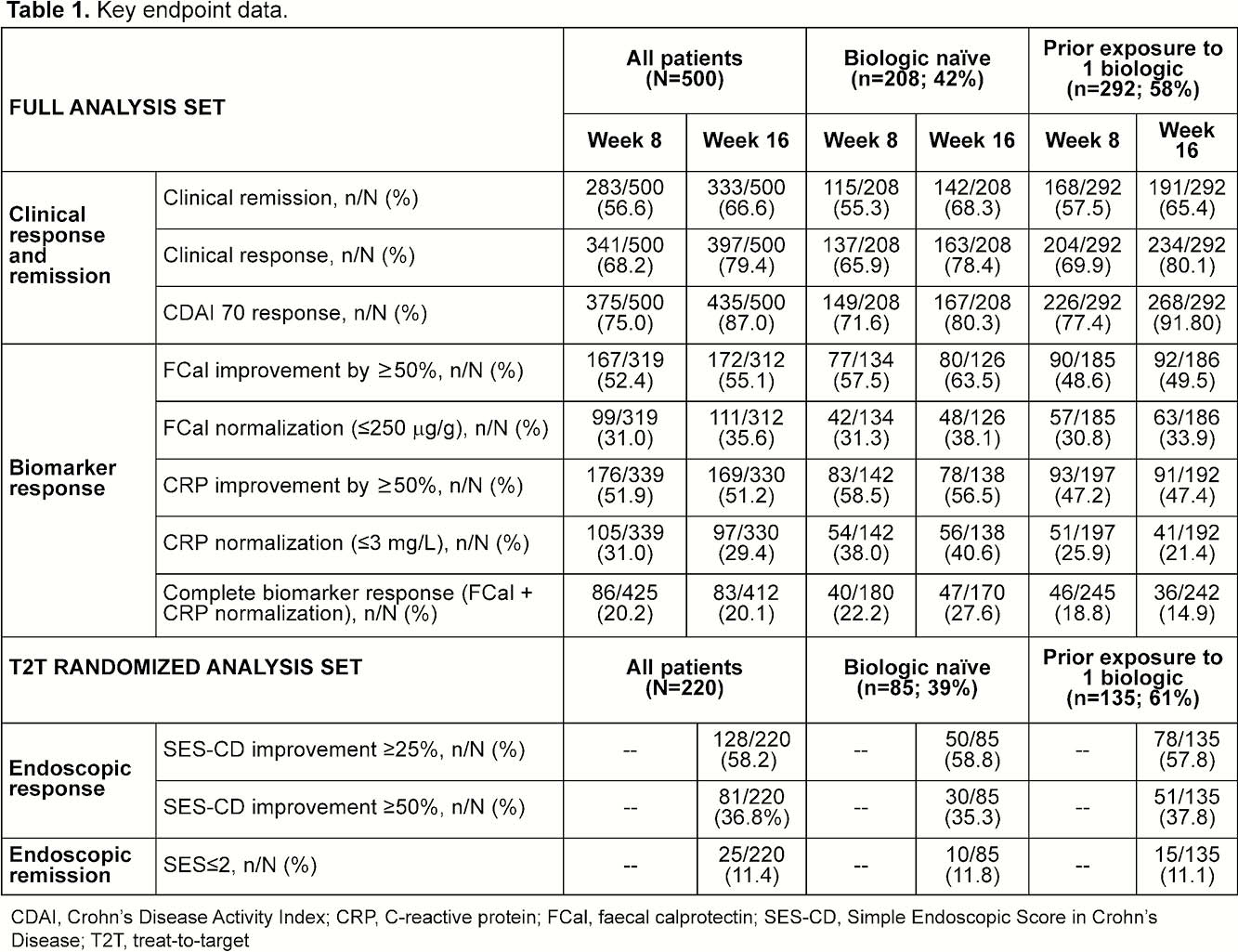
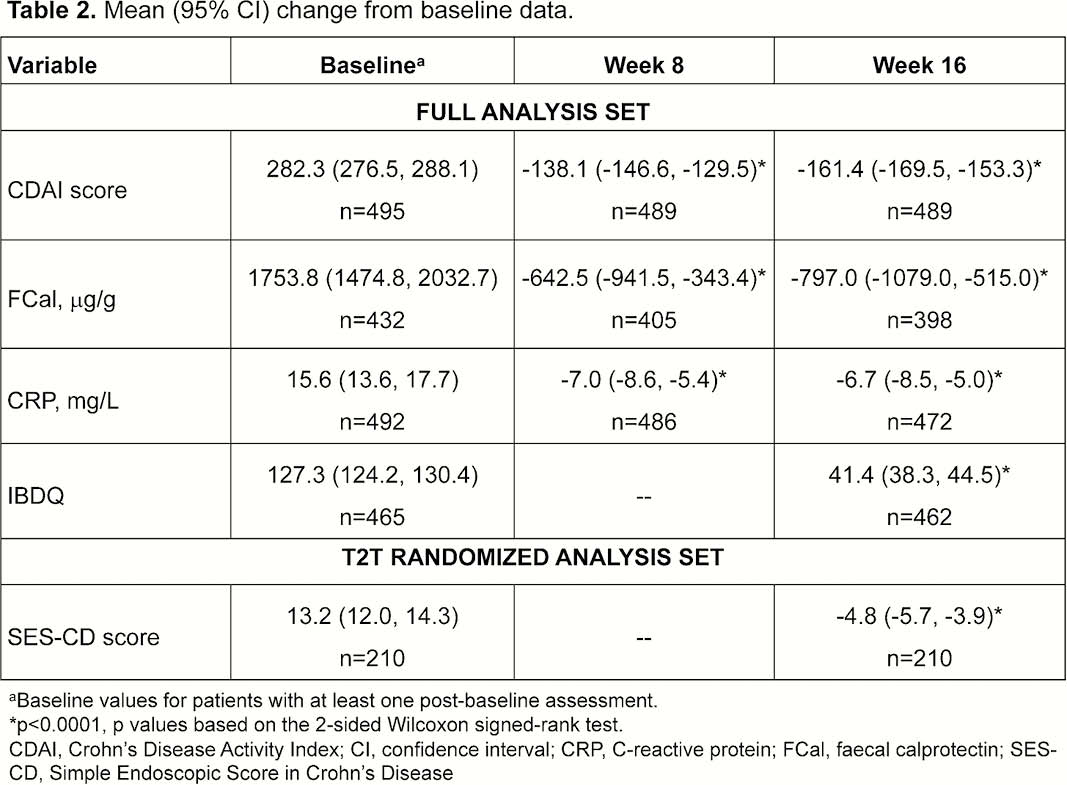
STARDUST, an ongoing phase 3b randomised strategy trial, enrolled adults with moderate–severely active CD (CD activity index [CDAI] 220–450) and simple endoscopic index for CD [SES-CD] ≥3) who failed conventional therapy ±1 biologic. At W0, patients received intravenous, weight-based UST of ~6mg/kg (approved label) and at W8, subcutaneous UST 90mg. At W16, patients with CDAI reduction ≥70 points were randomised (1:1) to T2T or standard of care. Key endpoints (intention-to-treat [ITT] set, as observed) were analysed at W8 and W16: % patients in clinical remission (CDAI score <150); % patients with a clinical response (CDAI <150 or decrease vs. baseline [BL] ≥100 points); faecal calprotectin (FCal) and C-reactive protein (CRP) levels: normalisation of FCal or/and CRP; improvement ≥50% vs. BL (patients with elevated FCal and CRP subpopulations); change vs. BL in CDAI and Inflammatory Bowel Disease Questionnaire (IBDQ) total scores. Patients randomised to T2T underwent colonoscopy at W16 and were analysed for change in SES-CD score vs. BL, endoscopic response (decrease in SES-CD score ≥50% vs. BL) and endoscopic remission (SES-CD score ≤2) (central reading).
Results
The ITT full set included 500 patients with BL mean (SD) CDAI score 282.3 (65.8), SES-CD 13.1 (8.1), CRP 15.7 (23.4) mg/l, FCal 1741.9 (2932.1) mg/g and disease duration 9.4 (8.7) years; 58.4% previously failed 1 biologic. At W16, 79.4% of patients had a clinical response and 66.6% were in clinical remission. About half of the patients showed ≥50% improvement in FCal and CRP levels, which normalised in about 1/3 of patients. Results were similar irrespective of previous biologic (Table 1); 84% of patients in response at W16 were in clinical remission. Statistically significant changes from BL in CDAI, FCal, and CRP were observed at W8, and in IBDQ scores at W16 (Table 2). In the T2T set (
Conclusion
STARDUST is the first T2T trial in CD patients. After 16 W following induction with UST, 2/3 of patients achieved clinical remission. Thirty-seven per cent of those randomised to the T2T arm (CDAI 70 responders) showed endoscopic response by central reading at W16. Results were similar irrespective of being bio-naïve or failing 1 biologic.