
DOP14 Modelling of the relationship between infliximab exposure, faecal calprotectin, and endoscopic remission in patients with Crohn’s disease
E. Dreesen1, S. Berends2, D. Laharie3, G. D’Haens4, S. Vermeire5, A. Gils1, R. Mathôt2
1Department of Pharmaceutical and Pharmacological Sciences, KU Leuven, Leuven, Belgium, 2Department of Hospital Pharmacy, Amsterdam UMC, Amsterdam, The Netherlands, 3Hepato-gastroenterology and Digestive Oncology, Haut-Lévêque Hospital- Bordeaux UMC, Bordeaux, France, 4Department of Gastroenterology and Hepatology, Amsterdam UMC, Amsterdam, The Netherlands, 5Department of Gastroenterology and Hepatology, University Hospitals Leuven, Leuven, Belgium
Background
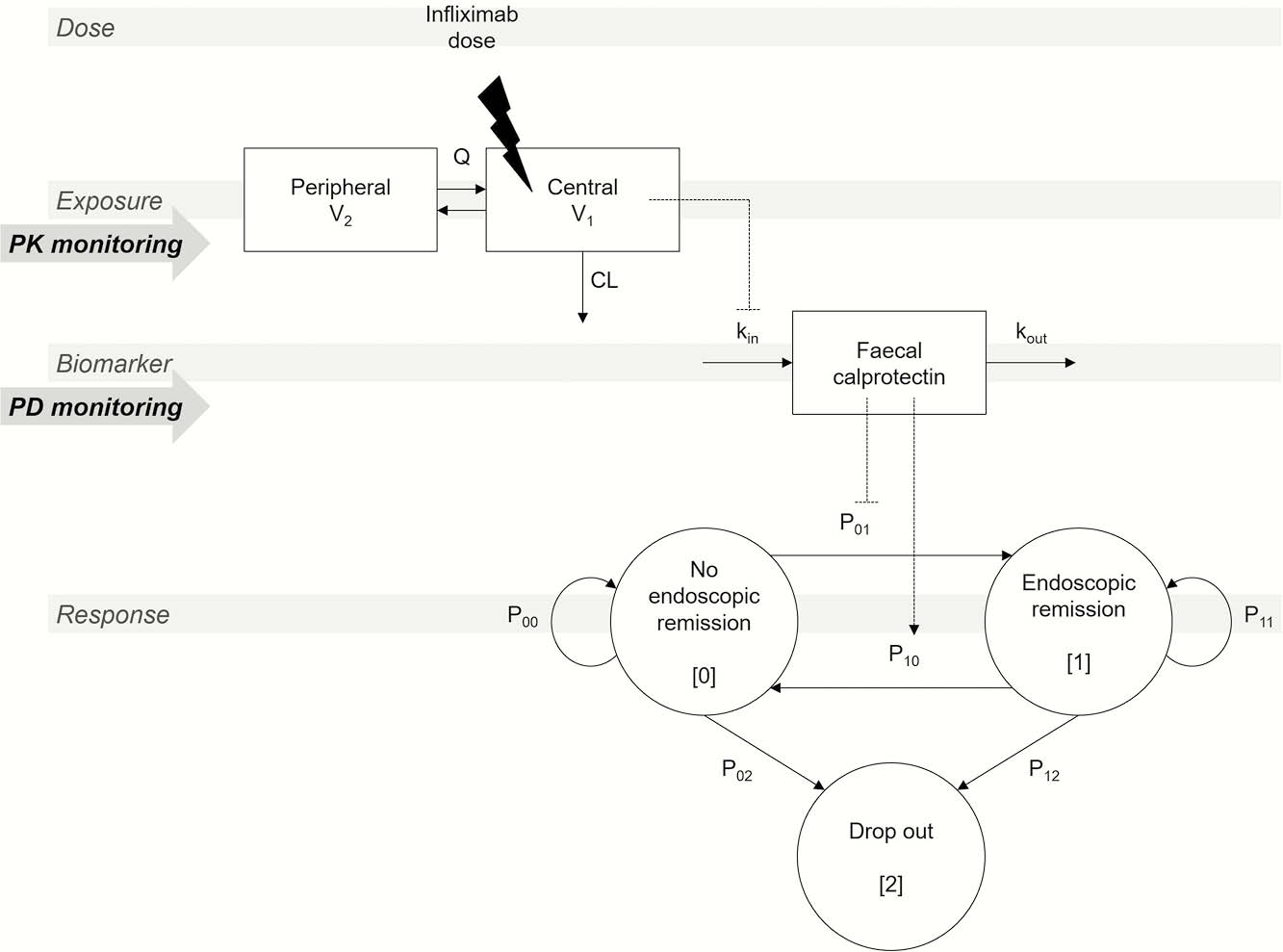
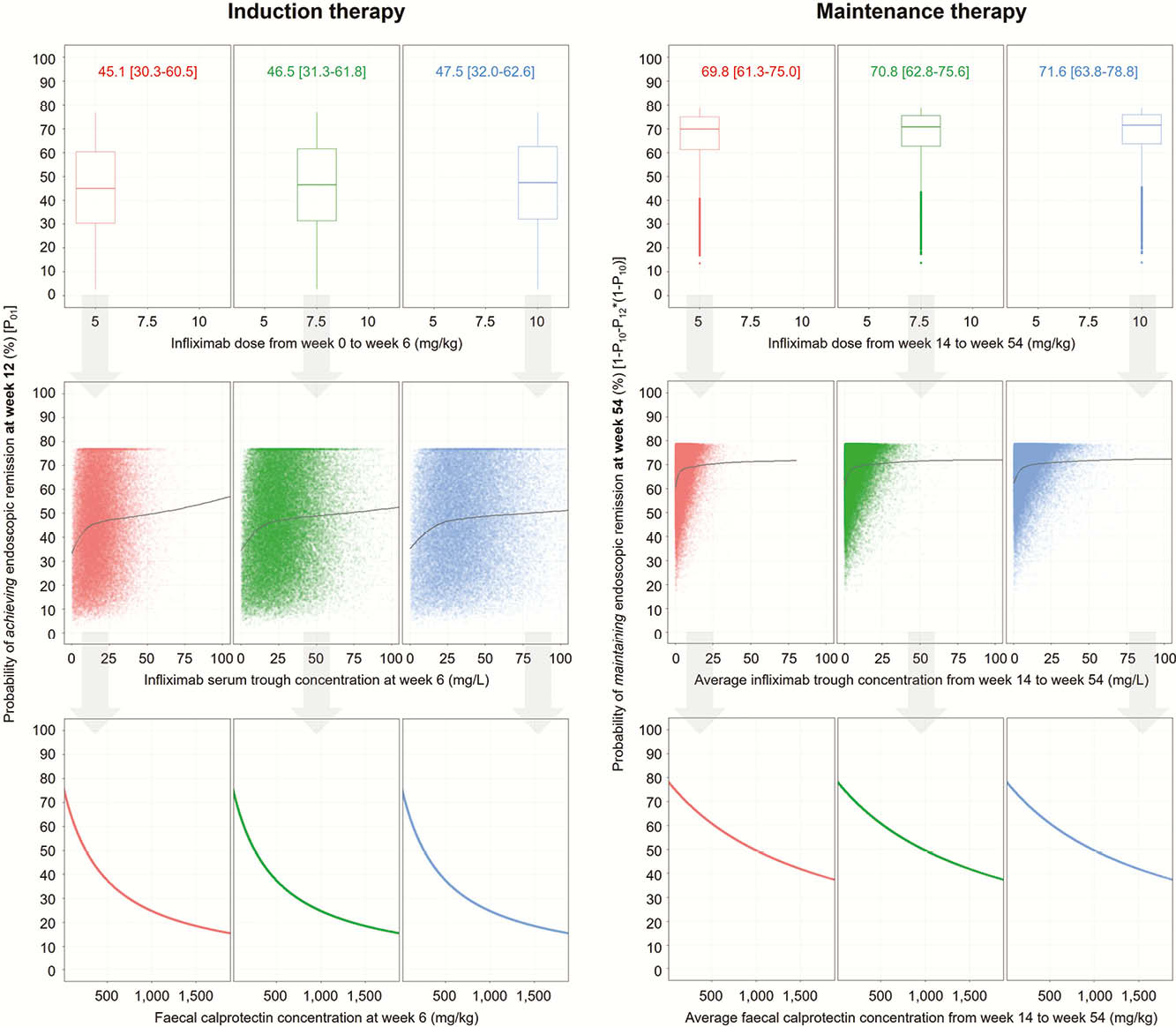
Less than 50% of patients with Crohn’s disease (CD) starting infliximab (IFX) therapy achieve endoscopic remission (ER). Evidence for the benefits of pharmacokinetic (PK) and pharmacodynamic (PD) monitoring remains scarce. We aimed to develop a population (pop)PK/PD model to characterise the IFX
Methods
Analyses were performed using data of a phase 4 dose-escalation study (TAILORIX). Patients started standard 5 mg/kg IFX induction therapy at weeks [w]0, 2 and 6. From w14 through w54, the IFX dose could be irreversibly doubled based on one of the three monitoring algorithms.1 Endoscopies were performed at w0, 12 and 54. Three sequential models were developed: A 2-compartment popPK model linking IFX dose to exposure, an indirect response popPK-PD model describing the inhibitory effect of IFX exposure on
Results
The study included 116/122 (95%) patients with CD enrolled in TAILORIX who had ≥1 detectable IFX serum concentration. In the developed models, it was shown that IFX clearance increased with increasing
Conclusion
Model-informed infliximab dose optimisation towards a predefined
D’Haens