
OP19 Disease course and treatment outcomes of early resected Crohn's Disease patients: A Danish nationwide cohort study from 1997 to 2015
Sarikaya, M.(1);Zhao, M.(2);Bendtsen, F.(1,2);Burisch, J.(2)
(1)University of Copenhagen- Copenhagen- Denmark, Faculty of Health Sciences, Copenhagen, Denmark;(2)Hvidovre University Hospital- Kettegaard Alle 30, The Gastro Unit- Medical Division, Hvidovre, Denmark
Background
Limited resective surgery is used as a primary therapeutic option in patients with Crohn’s disease (CD) who present with severe symptoms or fibrostenotic complications. Recent studies suggest that surgery represents a valid alternative of biological therapy in subgroups of CD patients.1 However, only few studies have described the disease course in early resected CD patients regardless of disease location. This study aimed to investigate disease course in all early resected CD patients.
Methods
Using the Danish National Patient Registry (NPR), we identified 9739 patients who were diagnosed with CD between January 1st, 1997 and December 31st, 2015. Of those, 499 patients underwent a major abdominal surgery within 30 days before or after their diagnosis. Data on re-operation, hospitalization and medication use were retrieved from the NPR and the National Prescription Registry. Trends in treatment outcomes over time were assessed using Chi-square test, Kaplan Meier survival analysis and log-rank test.
Results
Overall, 217 (43.5%) patients had an initial ileocecal resection, 154 (30.9%) had a colonic resection and 112 (22.4%) had a small bowel resection and 16(3.2%) patients without classification of surgery. The cumulative risk of reoperation was 16.4% at five years after the initial surgery. Five-year risk of hospitalization and need for medical therapy was 66.1% and 61.7% (Figure 1). Among 326 (65.3%) patients who received medical therapy during follow-up, 216 (66.3%) were treated with an immunomodulator and 62 (19.0%) with a biological drug. There was no difference in the risk of re-operation (p=0.11), hospitalization (p=0.70) or medication use (p=0.37) in relation to the anatomic location of the initial surgery.
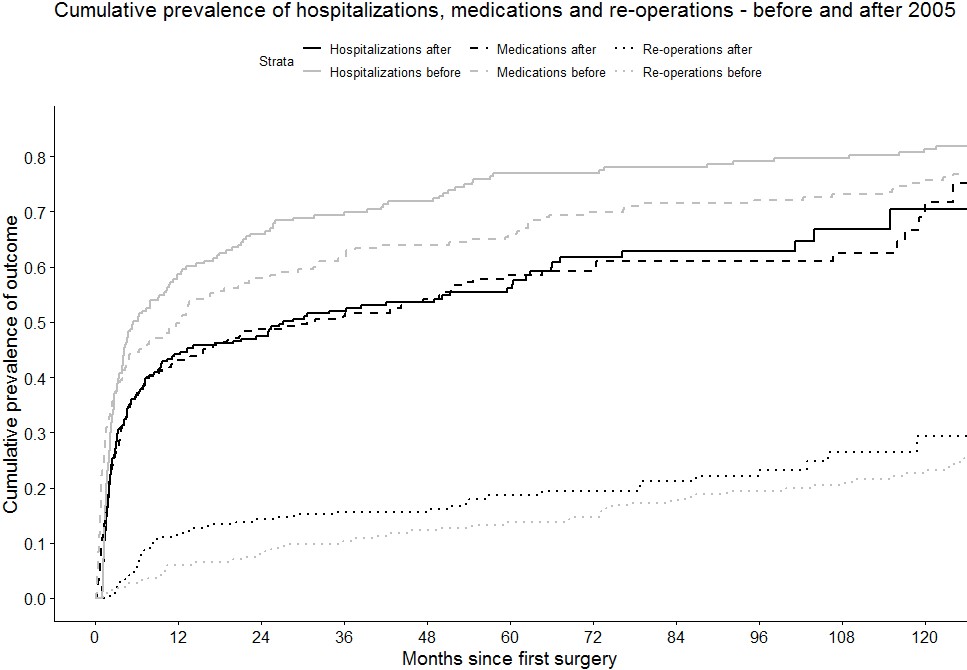
When comparing patients diagnosed before and after 2005, five-year risk of hospitalization decreased from 76.9% to 56.1% (p<0.001, Figure 2), while five-year risk of medication use decreased from 65.9% to 58.5% (p=0.01, Figure 2). In contrast, five-year risk of re-operation showed an increasing, but insignificant trend from 13.7% to 18.6% (p=0.18).
Figure 1. Cumulative risk of re-operation, hospitalization and medication use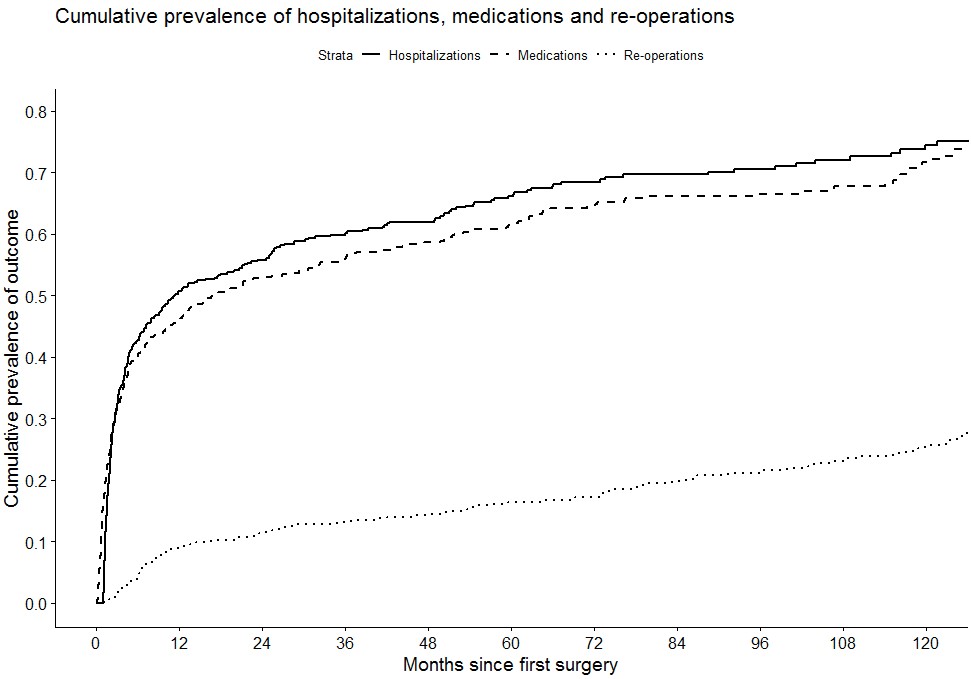
Conclusion
The risk of re-operation and hospitalization after the initial surgery in this cohort of early resected CD patients are lower when compared to other CD cohorts. Furthermore, hospitalization risk and need for medical therapy decreased over time.
1.Stevens TW, Haasnoot ML, D’Haens GR, Buskens CJ, de Groof EJ, Eshuis EJ, et al. Laparoscopic ileocaecal resection versus infliximab for terminal ileitis in Crohn’s disease: retrospective long-term follow-up of the LIR!C trial. Lancet Gastroenterol Hepatol. 2020 Oct 1;5(10):900–7.