
OP21 Positivity thresholds of total infliximab and adalimumab anti-drug antibody assay: The prevalence of clearing and transient anti-drug antibodies in a national therapeutic drug monitoring service
R. Nice1, N. Chanchlani2, H. Green2, C. Bewshea2, N. Kennedy2, T. Ahmad2, J. Goodhand2, T. McDonald1, M. Perry1
1Department of Blood Sciences, Royal Devon and Exeter Hospital, NHS Foundation Trust, Exeter, UK, 2Exeter IBD Pharmacogenetics, University of Exeter., Exeter, UK
Background
Anti-drug antibodies can affect biopharmaceutical pharmacokinetics by increasing or decreasing drug clearance. Drug-tolerant (total), unlike drug-sensitive (free), antibody assays permit antibodies to be measured in the presence of a drug. We sought to confirm the positivity threshold of our total anti-tumour necrosis factor (TNF) antibody ELISA assays in a sample of healthy volunteers and to use this threshold to report the prevalence of clearing and transient antibodies in patients treated with infliximab and adalimumab.
Methods
Serum was obtained from a random sample of 498 anti-TNF-naïve healthy adults recruited to the Exeter Ten Thousand study and tested for total anti-drug antibodies to infliximab and adalimumab. Using recommendations for confirmatory anti-drug antibody validation, we used bootstrapping to calculate the 80% one-sided lower confidence interval [CI] of the 99th centile to define assay thresholds.
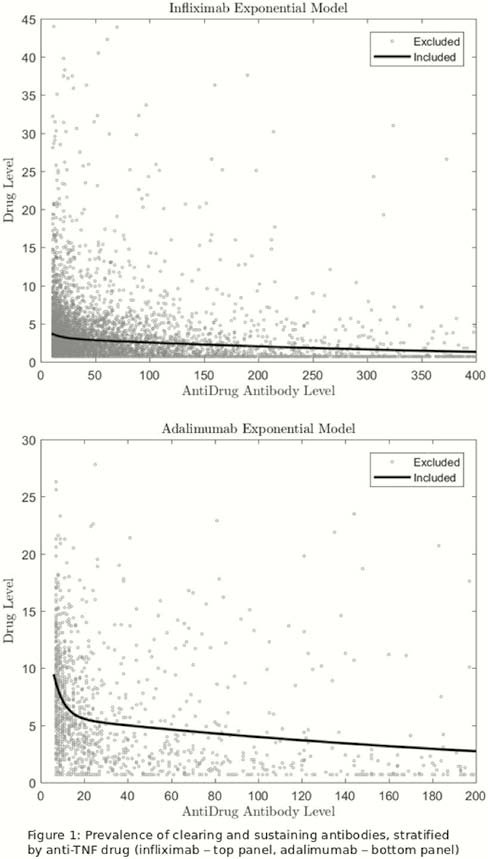
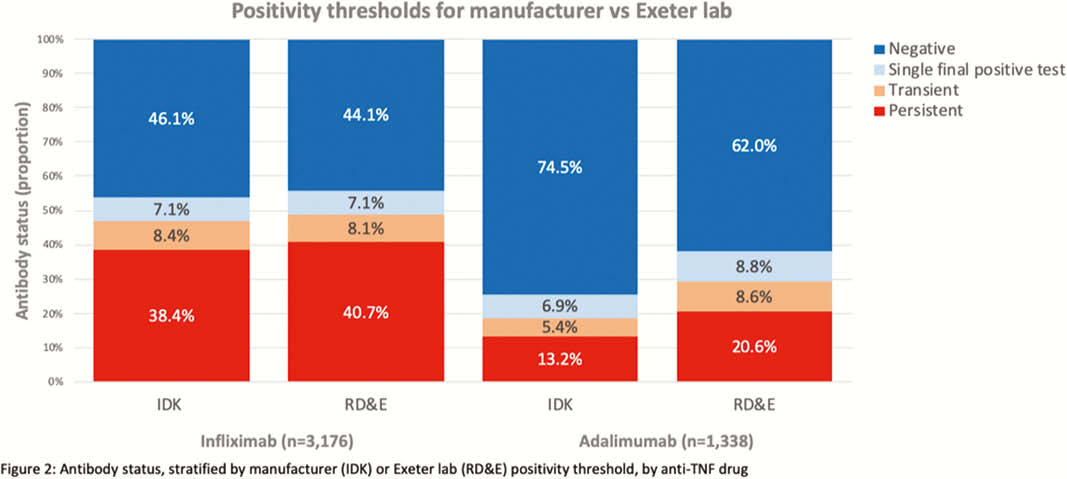
We used paired drug and anti-drug antibody levels derived from our national therapeutic drug monitoring service to report the distribution of clearing (antibody positive, drug negative) vs. non-clearing (antibody positive, drug positive) antibodies. In patients with at least two test results, antibodies were classified as transient (single positive test with subsequent negative test) or persistent (at least two positive tests).
Results
The 80% one-sided lower CI of the 99th centile titre for total anti-drug antibody to infliximab and adalimumab were 8.7 AU/ml and 5.9 AU/ml, respectively. Using the manufacturer’s recommended threshold of 10 AU/ml for both total anti-TNF antibody assays, in healthy individuals, the prevalence of positive antibodies to infliximab and adalimumab was 1% (5/498) and 0.2% (1/498), respectively. Using the manufacturer’s threshold, at the time of last testing, of 7447 and 4054 patients treated with infliximab and adalimumab; 20.9% (
Conclusion
We report lower positivity thresholds for the IDKmonitor® total anti-TNF antibody ELISA assays than the manufacturer, in particular, for adalimumab. Transient antibody formation is uncommon: most patients develop persistent anti-drug antibodies that lead to drug clearance.