
P023 Immune-metabolic profiles of creeping fat in relation to degree of severity in Crohn's disease postsurgical recurrence.
Suau, R.(1,2)*;Pardina, E.(3);López-Tejero, M.D.(3);Lorén, V.(1,2);Zabana, Y.(2,4);Llaves, M.(1);Cordobilla, B.(3);Cañete, F.(2,5);Guasch, M.(6);Ricart-Jané, D.(3);Mañosa, M.(2,5);Domènech, E.(2,5);Domingo, J.C.(3);Manyé, J.(1,2);
(1)Institut d'Investigació Germans Trias i Pujol IGTP, IBD Research Group, Badalona, Spain;(2)Centro de Investigación Biomédica en Red, Enfermedades Hepáticas y Digestivas CIBEREHD, Madrid, Spain;(3)Universitat de Barcelona, Biochemistry and Molecular Biology Department, Barcelona, Spain;(4)Hospital Universitari Mútua Terrassa, Gastroenterology Departament- IBD Unit, Terrassa, Spain;(5)Hospital Universitari Germans Trias i Pujol HUGTP, Gastroenterology Department, Badalona, Spain;(6)Hospital Parc Sanitari Sant Joan de Déu, Surgery Department, Sant Boi de Llobregat, Spain;
Background
Crohn’s disease (CD) is an inflammatory bowel disease (IBD) of complex etiology that normally requires bowel resection. However, many patients suffer from post-operative recurrence (POR) within one year. Here, the inflammatory and bacterial influence of the affected intestine transforms the neighboring mesenteric tissue to creeping fat (CrF). The main objective has been to characterize the immune-metabolic profile of CrF according to the POR severity and compare them with mesenteric tissues from IBD-free controls (colorectal cancer and severe obesity).
Methods
POR severity was classified using the Rutgeerts index: non-recurrents (i0+i1, n=18; NR), mild-recurrents (i2, n=14; MR) and severe-recurrents (i3+i4, n=10; SR). The CrF were gathered from intestinal resections, and IBD-free mesenteric tissues were collected from intestinal resections for colorectal cancer (n=10) and bariatric surgery for severe obese patients (n=11). The total DNA was quantified using DABA assay, 105 cytokines were semiquantified by immune blotting and the fatty acid (FA) profile was quantified by GC-MS.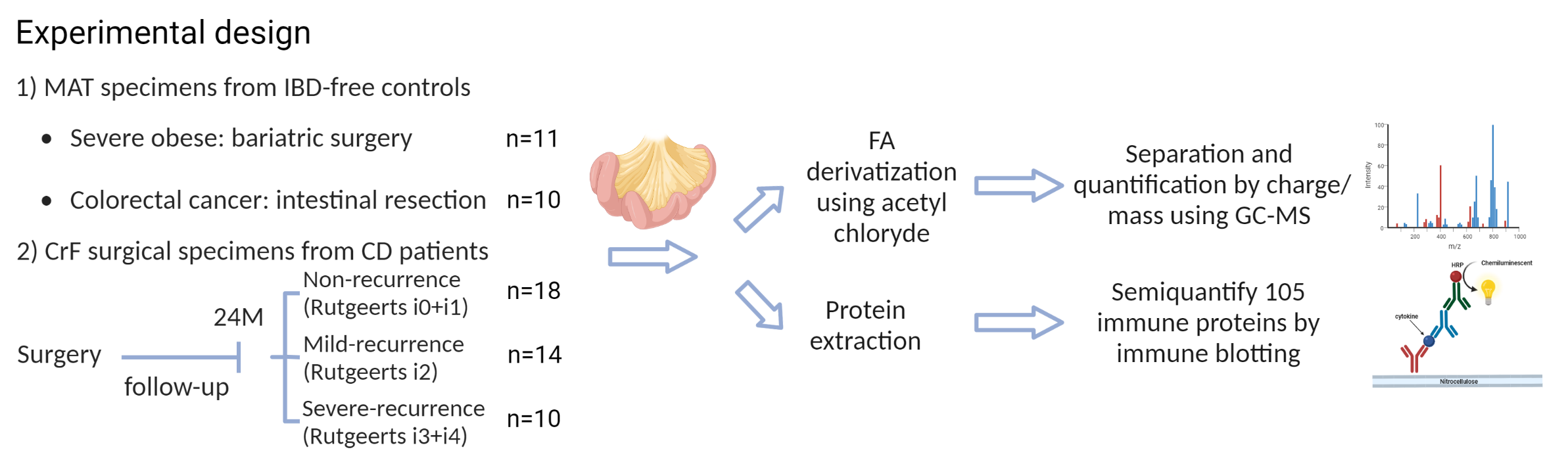
Results
The DNA analyses in the CrF showed a major cellularity demonstrating the hyperplasia. When compared to the control groups and to SR, the NR patients showed an increment of infection pro-resolutive cytokines (IFN-γ, MIF, BAFF), and, specially, an increase in both Th1 and Th2 cytokines (IL-18, IL-33). Here, there was also an increase in molecules related to angiogenesis (endoglin) and cellular adhesion (ICAM-1 and VCAM-1). On the other hand, the SR showed a higher level of pro-fibrotic PAI-1 and of the leukocyte homing inducer CCL5.
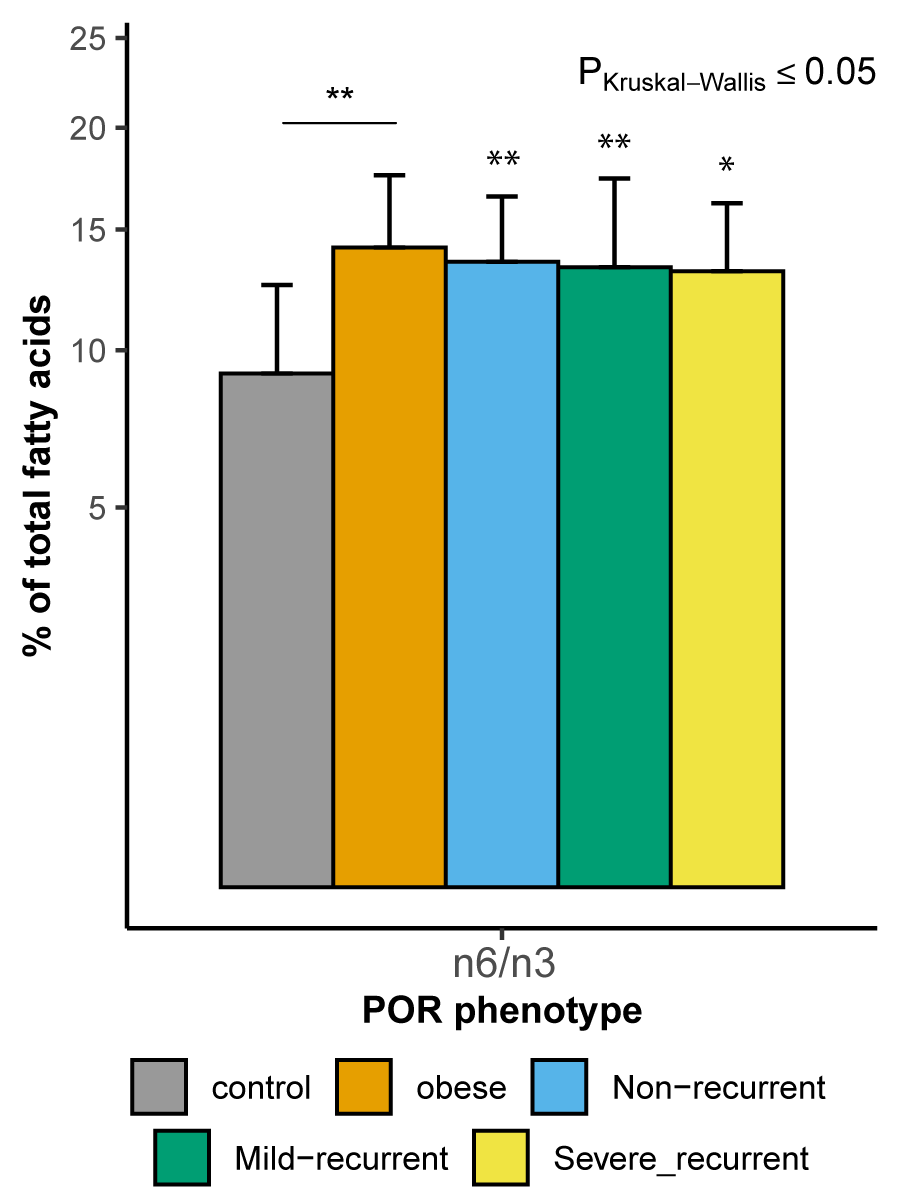
Going into the FA, in comparison to the control groups, there was an increase in the saturated in front of a decrease in mono-unsaturated FA in all the CD groups. Regarding the polyunsaturated FAs, the CrF and the obese mesentery showed a general increase of the omega 6/omega 3 FA ratio when compared to colorectal cancer controls.
Finally, both obese and NR CD patients had less short-chain FAs, specifically acetate and propionate, than the colorectal controls. Unexpectedly, the butyrate levels were very low in all the mesenteric tissues.
Conclusion
The CrF from NR CD patients show an infection resolutive profile regarding the controls and the SR. Instead, these lasts showed signs of chronic inflammation and a fibrotic profile. In general, CrF FA proportions suggests changes in cell signaling due to loss of cell membrane fluidity. In addition, the greater presence of omega-6 than omega-3 FA in the CrF and mesentery of obese patients could be related to the generation of potent proinflammatory lipid mediators. In contrast, the propionate and acetate decrease detected in NR CD patients could be protective against POR.