
P026 Inflammatory bowel disease does not preclude the presence of environmental enteropathy in Zambian adults
Hodges, P.(1);Mulenga, C.(2);Banda, R.(2);Kelly, P.(1);
(1)Queen Mary University of London, Blizard Institute- Barts and the London School of Medicine and Dentistry, London, United Kingdom;(2)University of Zambia School of Medicine, Tropical Gastroenterology and Nutrition Group, Lusaka, Zambia;
Background
Although data is scarce, inflammatory bowel disease (IBD) seems to be increasing in incidence in newly industrialised countries.(1) The environmental factors driving this change are not entirely clear, although it seems likely that changing diet and improving hygiene and sanitation are involved. In China, incidence of IBD is positively associated with gross domestic product.(2)
Environmental enteropathy (EE) is a lesion of the small bowel with villous blunting, chronic inflammation and increased gut permeability seen in people living in insanitary conditions in resource-limited settings. We set out to examine whether EE would be present in patients with IBD in Zambia, as these individuals are likely to come from higher socioeconomic strata hence would be expected to live in more sanitised environments. Here we report preliminary data.
Methods
IBD cases were recruited at time of diagnosis or follow-up. Two groups of controls were recruited: individuals of higher socioeconomic status attending the GI clinic for investigation of symptoms of dyspepsia who had normal upper GI endoscopy were recruited to control group A, and healthy individuals from Misisi compound where studies on EE have been conducted over the past two decades to control group B (low socioeconomic status). All participants gave informed consent and underwent upper GI endoscopy and collection of duodenal biopsies. Haematoxylin- and eosin-stained sections of paraffin-embedded formalin-fixed biopsies were imaged on an Olympus VS120 scanning microscope then assessed for villous height, crypt depth, and epithelial surface area. Demographic information was collected via questionnaire.
Results
Biopsies were collected from 13 cases, 7 controls in group A and 10 controls in group B. Demographics are shown in Table 1. Cases and controls in group A had a higher number of rooms in the house than controls in group B but there was no significant difference in other environmental factors. Other than crypt depth, which was greater in controls from the lower socioeconomic group, there was no significant difference in morphometric parameters between IBD cases and controls (Table 2). The most severe enteropathy is seen in the biopsy from control group B (Figure 1c) which is made up of participants recruited a socioeconomically deprived district of Lusaka.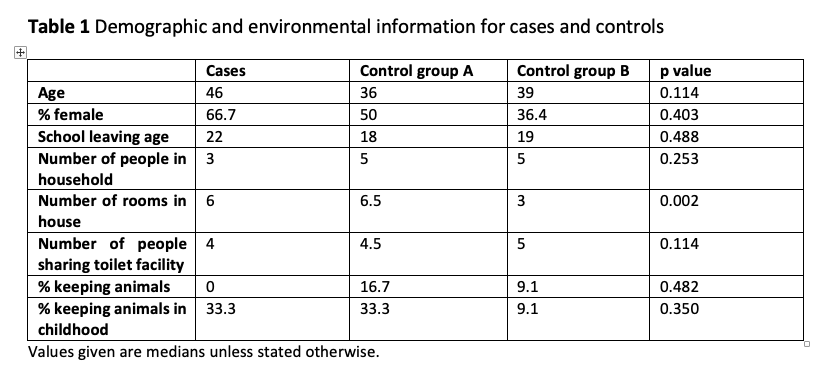

Figure 1
Conclusion
EE can coexist alongside IBD, suggesting that immunological drivers of these conditions are not distinct, and do not support the hygiene hypothesis. There is evidence of some degree of EE in small bowel biopsies from all cases and controls. Normal villous height to crypt depth ratio is likely to be between 3 and 5 (3) whereas medians for villous height:crypt depth in all groups in this study were less than 2.