
P111 Elucidation of inflammatory infiltration of myenteric plexus in IBD
J.J. Wiese, A. Fascì, A.A. Kühl, B. Siegmund, M.S. Prüß, M. Schumann
Department of Gastroenterology, Infectious Diseases and Rheumatology, Campus Benjamin Franklin, Charité – Universitätsmedizin Berlin, Berlin, Germany
Background
Since IBD is frequently associated with chronic abdominal pain and visceral hypersensitivity, affections to the sensory nerves within the ENS appear to be pivotal. In both inflammatory bowel diseases, i.e. the transmural inflammation of Crohn’s disease (CD) and the inflammation restricted to the colonic mucosa in ulcerative colitis (UC) infiltrations of the plexus by immune cells occur. However, the type of immune cells involved is so far unknown. Therefore, we characterised the immune cell infiltrations of myenteric plexus (MP) in CD and UC compared with controls.
Methods
We identified 12 IBD patients (four CD and eight UC) and four controls that had received surgery (ileocecal resections or colectomy). The severity of the disease was assessed by Mayo score, HBI score and questionnaires (Visual Analogue Scale, Pain Catastrophizing Scale, Inflammatory bowel disease quality of life and Irritable Bowel Symptom Severity Scale). Formalin-fixed, paraffin-embedded tissue was stained by classical immunohistochemistry. To identify myenteric plexus tissue was stained for CGRP and PGP9.5. Immunostainings for immune cells (T cells: CD3, CD4, CD8, Foxp3; B cells: CD20; monocytes/macrophages: CD68 and CD163) were analysed by quantifying within the plexus and within a defined area of 100 µm around the plexus.
Results
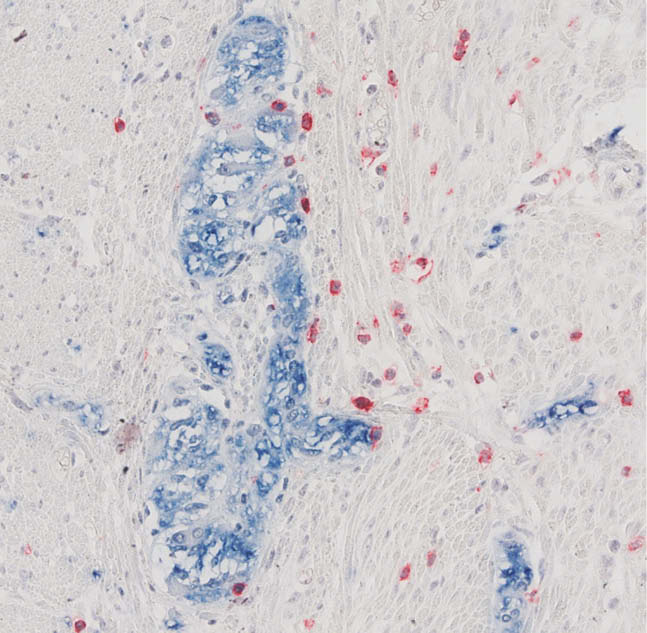
The mean size of myenteric ganglia in controls was found to be 0.100 ± 0.004 mm² and was significantly decreased in CD (0.055 ± 0.002 mm²) and UC (0.079 ± 0.004 mm²). The population of CD4+ T-cells, macrophages and monocytes within ganglia of the MP were unchanged in CD, UC. However, infiltrates within and around MP contained significantly more CD3+ T cells in CD (121 ± 63 intraganglionic cells/mm² and 1858 ± 1133 periganglionic cells/mm²) and UC (133 ± 80 intraganglionic cells/mm² and 1198 ± 693 periganglionic cells/mm²) compared with controls (28 ± 38 intraganglionic cells/mm² and 342 ± 93 periganglionic cells/mm²). This appeared to be secondary to a significant increase of periganglionic CD8+ T cells in UC (342 ± 293 cells/mm² compared with 164 ± 140 cells/mm² in controls) (see Figure 1) and secondary to a significant increase of periganglionic Foxp3+ T cells in CD (528 ± 193 cells/mm² compared with 0 ± 0 cells/mm² in controls). Moreover, CD20+ B cells were significantly increased in CD (528 ± 193 periganglionic cells/mm² compared with 0 ± 0 periganglionic cells/mm² in controls).
Conclusion
The intra- and periganglionic infiltrate of MP in inflammatory bowel disease contains CD3+CD8+ T cells in UC and CD3+Foxp3+ regulatory T cells as well as B cells in CD.