
P130 Faecal calprotectin is a reliable tool to assess endoscopic activity in ulcerative colitis except for short-extent proctitis
R. Collin, R. Minet-Quinard, L. Blayac, L. Manlay, B. Pereira, A. Buisson
CHU Estaing, Department of Digestive and Hepatobiliary Medicine, Department of Gastroenterology, Clermont-Ferrand, France
Background
Faecal calprotectin (Fcal) is now considered a reliablebiomarker of endoscopic inflammatory activity in patients with ulcerative colitis (UC). However, this biomarker remains imperfect with some false negative in some clinical situations. We aimed to search for endoscopic factors associated with faecal calprotectin level in patients with UC and to identify situations in which this tool might be less efficient.
Methods
From a database collecting consecutively all the patients with IBD with at least one Fcal dosage in our centre between June 2016 and June 2018, we included all patients who had an endoscopic evaluation within the month before or after dosing without intervention therapeutic during this interval. Fcal level was measured by immuno-chemiluminescence in all patients.
Results
One hundred and thirty-four patients were included (E1 in 12 patients (9.0%), E2 in 69 patients (51.5%) and E3 in 53 of them (39.5%)). There was a significant correlation between the UCEIS score and Fcal level (
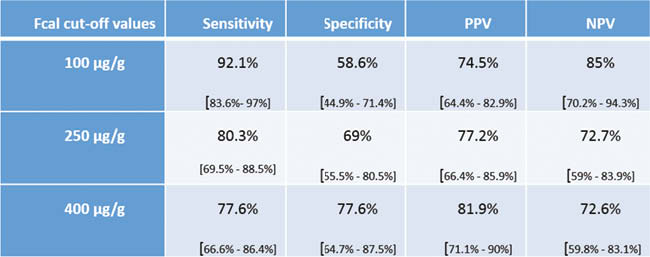
In the same way, 100 μg/g was the best Fcal threshold to define a remission endoscopic (endoscopic Mayo score = 0): sensitivity = 79.3% [66.6%–86.3%], specificity = 88.9% [65.3%–98.6%], PPV = 97.9% [92.5%–99.7%], VPN = 40% [24.9%–56.7%]. In multivariate analysis, endoscopic factors associated with the values of CF are: the UCEIS sub-score – vascular pattern (
Conclusion
CF is a reliable tool for indirect and non-invasive assessment of activity endoscopic inflammatory disease in UC. Fcal is mainly influenced by severity and extent of the lesions. Its use should be careful in case of proctitis under 5 cm, a situation in which its performances are more questionable.