
P140 Factors associated with development of NAFLD in patients with inflammatory bowel disease: a 5-year retrospective study on 225 patients
V. Domislović1, I. Knežević-Štromar1,2, M. Premužić1, M. Brinar1,3, D. Vranešić Bender4, A. Milinković3, M. Matašin3, I. Mikolašević5,6, Ž. Krznarić1,2,4
1Clinical Hospital Centre Zagreb, Department of Gastroenterology and Hepatology, Zagreb, Croatia, 2Zagreb School of Medicine, Department of Gastroenterology and Hepatology, Zagreb, Croatia, 3Zagreb School of Medicine, University of Zagreb, Zagreb, Croatia, 4Unit for Clinical Nutrition, Department of Gastroenterology and Hepatology, Zagreb, Croatia, 5Clinical Hospital Merkur, Department of Gastroenterology and Hepatology, Zagreb, Croatia, 6School of Medicine Rijeka, University of Rijeka, Rijeka, Croatia
Background
Patients with IBD are at higher risk for non-alcoholic fatty liver disease (NAFLD) comparing to general population. Complex pathogenesis of NAFLD in IBD may be related to disease-specific risk factors such as chronic inflammation, steroid exposure, drug induced hepatotoxicity, malnutrition and alteration of gut microbiota, which is emerging as a major factor in the pathogenesis of NAFLD. The goal of the study was to investigate factors associated with NADLF and advanced liver fibrosis (ALF) in patients with CD and UC.
Methods
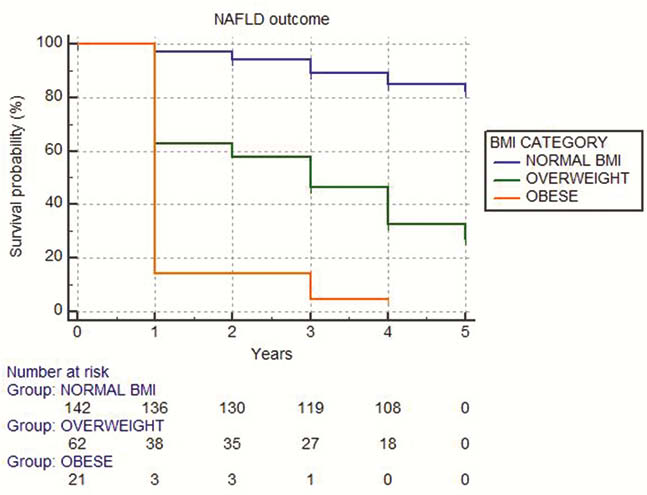
This is a retrospective study on IBD patients without extraintestinal manifestations and known liver disease. NAFLD was defined as Hepatic Steatosis Index (HSI) ≥ 36, and ALF was defined as FIB-4 ≥ 2.67. Predictors of NAFLD development were analysed using Kaplan–Meier and Cox regression analyses.
Results
In this retrospective study, we have included 225 IBD patients; 72.4% (
Conclusion
NAFLD is frequent comorbidity in patients with CD and UC, which can lead to development of advanced liver fibrosis. Our results show that patients with IBD have a high risk of NAFLD development, whereas the increased risk for ALF was not observed. Overweight and obese patients and those with dyslipidemia should be closer monitored due to significantly higher risk of NAFLD. This study points out the complexity disease-specific risk factors and importance of better stratifying IBD patients at risk of NAFLD and advanced liver fibrosis.