
P207 Modelling 1-year surgery risk in Crohn’s disease: A retrospective cohort study
J. Yao, X. Peng, Y. Jiang, M. Zhi
Department of Gastroenterology, Guangdong Provincial Key Laboratory of Colorectal and Pelvic Floor Disease, The Sixth Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China
Background
Accelerated therapeutic treatment should be considered in patients with progressive Crohn’s disease (CD) to prevent complications as well as surgery. Therefore, screening for risk factors and predicting the need for early surgery is of great importance in clinical practice. We aimed to establish a model to predict CD-related early surgery.
Methods
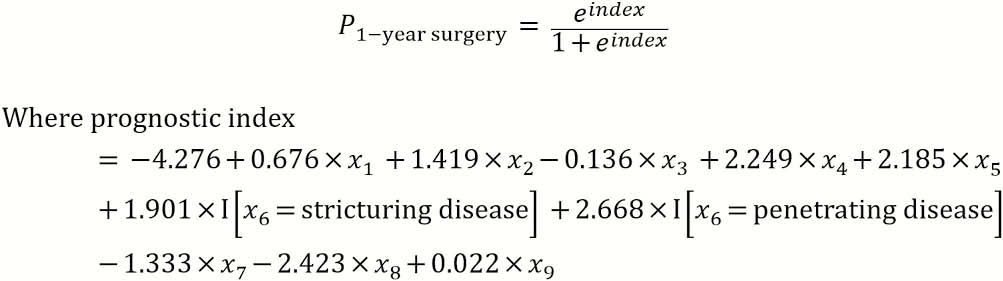
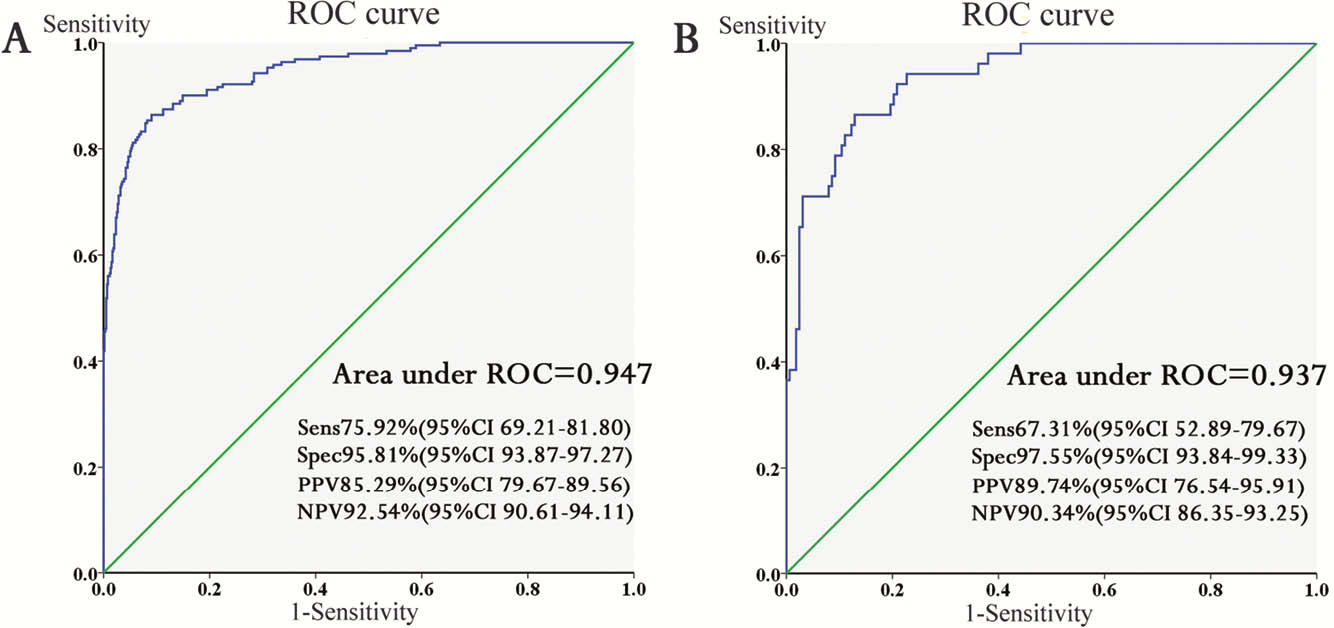
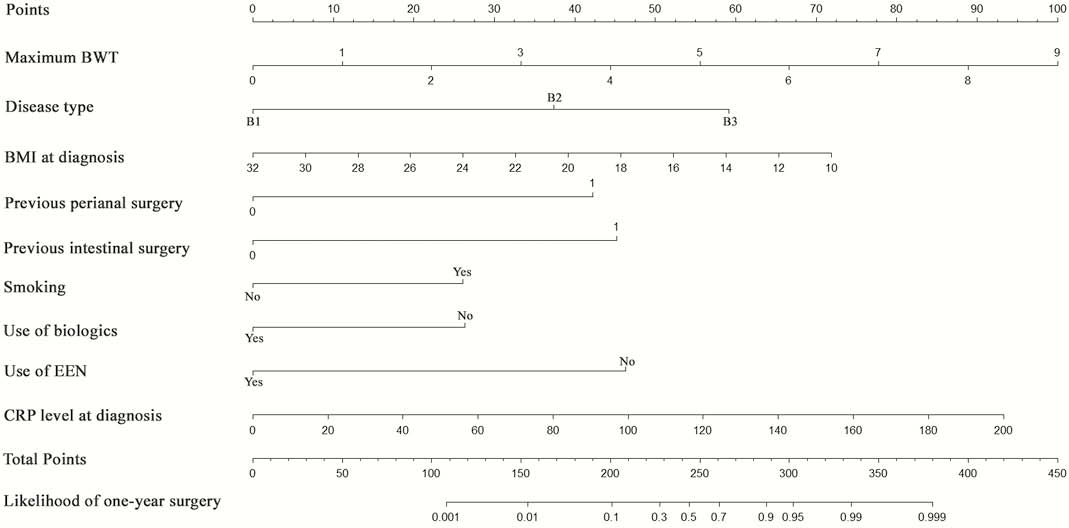
This was a retrospective study collecting data from CD patients diagnosed in our inflammatory bowel disease (IBD) centre from 1 January 2012 to 31 December 2016. All data were randomly stratified into a training set and a validation set at a ratio of 8:2. Multiple logistic regression analysis was conducted with receiver operating characteristic (ROC) curves constructed and areas under the curve (AUC) calculated. This model was further validated with a nomogram developed.
Results
A total of 1002 eligible patients were enrolled with a mean follow-up period of 53.54 ± 13.10 months. In total, 24.25% of patients received intestinal surgery within 1 year after diagnosis due to complications or disease relapse. Disease behaviour (B2: OR 6.693,
Conclusion
This prognostic model can effectively predict 1-year risk of CD-related intestinal surgery, which will assist in screening progressive CD patients and aid in tailoring therapeutic management.