
P243 Relationship between intestinal ultrasound, fecal calprotectin and Harvey-Bradshaw Index in the assessment of infllamatory activity in Cronh´s Disease
Montero Moretón, Á.M.(1);Bastón Rey, I.(2);Calvino Suarez, C.(2);De la Iglesia García, D.(2);Ferreiro Iglesias, R.(2);Maestro Antolín, S.(1);Santos Santamarta, F.(1);Pérez Millán, A.G.(1);Dominguez-Munoz, E.(2);Barreiro-de Acosta, M.(2);
(1)Complejo Asistencial Universitario de Palencia, Gastroenterology, Palencia, Spain;(2)Hospital Clínico Universitario de Santiago, Gastroenterology, Santiago de Compostela, Spain;
Background
Crohn's disease (CD) is an inflammatory bowel disease with chronic course and exacerbations. Diagnosis and follow-up are based on clinical activity, biomarkers, ileocolonoscopy and imaging techniques. Intestinal ultrasound (IUS) has been shown to have high sensitivity and specificity analyzing inflammatory activity in CD. The aim of our study is to correlate IUS parameters with clinical activity and biomarkers in CD.
Methods
Retrospective, observational, single-center study was designed. Adult patients with CD who underwent IUS between September 2020 and May 2021 were included. Exclusion criteria was exclusive colonic involvement. Examination was done by ultrasound machine (Hitachi Ascendus) with low frequency curved-array (1-5 MHz) and high-frequency linear-array (5-13 MHz) transducers. Examination assessed bowel wall thickness, mesenteric fat hypertrophy, lymph nodes, hyperemia on color Doppler flow measured as Limberg index and length of affected segment (cm). Clinical activity score for CD was assessed by Harvey Bradshaw index (HBI). Biomarkers parameters studied were C-reactive protein (CRP) and faecal calprotectin (FC).
Results
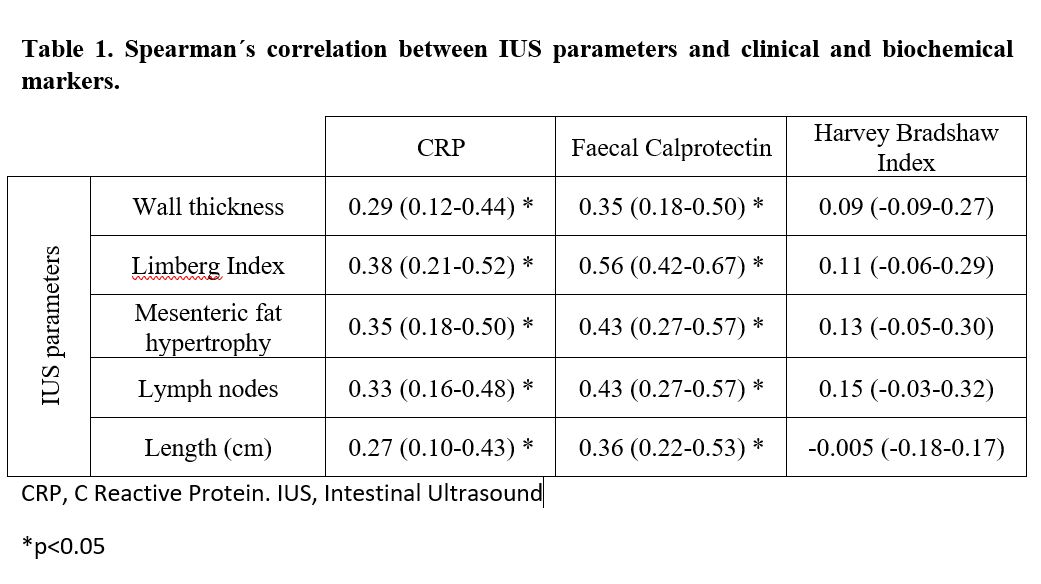
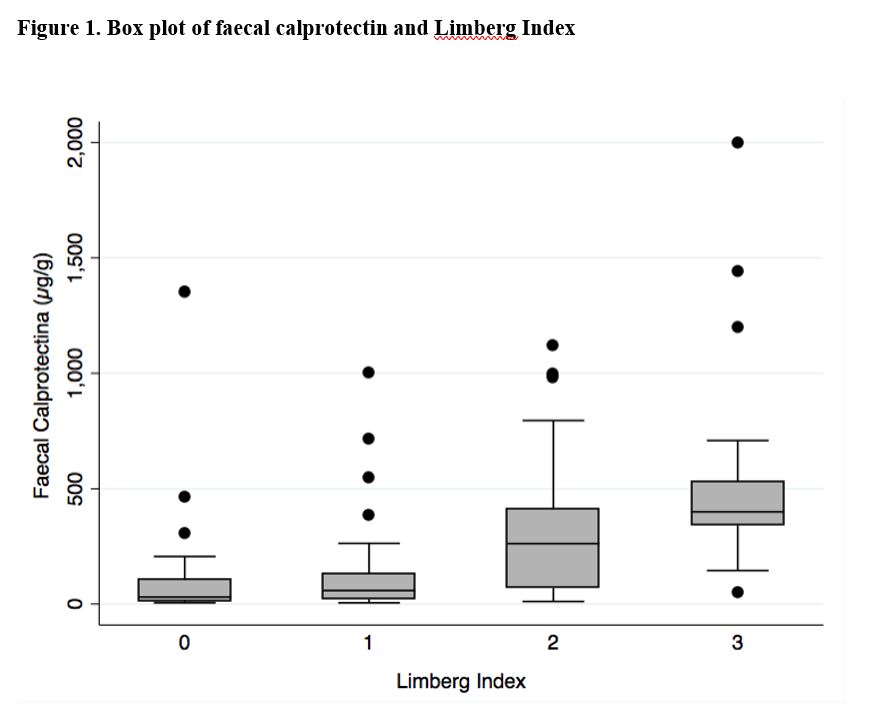
Results are shown as percentages, median and interquartile range (IQR). Data were analysed using Spearman´s correlation analysis121 patients were included (median age 45.6 years (IQR 33.4 – 59.6), 56.2% female). 78.5% had ileal disease and 21.5% ileocolonic involvement. At the time of IUS 17.4% of patients were not taking any maintenance treatment, 13.2% were on azathioprine, 48.8% on anti-TNF (61% adalimumab; 39% infliximab) and 8.3% on ustekinumab. 85.1% patients had HBI <6, 14.1% had moderate activity. Median CRP level was 0.334 mg/dl (IQR 0.06-1.12), FC was 141 µg/g (IQR 35-386). Median wall thickening was 4.7 mm (range 4.1-5.6), 68.6% of patients had mesenteric fat hypertrophy and 73.55% had lymph nodes. Limberg index was 0 in 20.7%, 1 in 23.1%, 2 in 37.2% and 3 in 19% of patients. IUS determined treatment modification in 60.3% of cases: 19% started biological therapy, 15.7% changed biological target, 14.9% underwent intensification or reinduction of biological treatment, in 1.7%, treatment reduction was decided. The Spearman´s correlation between IUS parameters, clinical and biochemical markers is presented in Table 1. IUS parameters were significantly associated with faecal calprotectin and CRP level, specially Limberg Index and faecal calprotectin (r=0.56, p<0.05) and Limberg Index and CRP level (r= 0.38, p<0.05) (Figure 1 and 2). No correlation was observed between HBI and IUS parameters.

Conclusion
Through this study, significant correlation between IUS and biomarkers was observed in CD. IUS has been shown to be useful for monitoring CD activity in order to optimize patients´ treatment.