
P261 Systematic review with meta-analysis: The impact of concomitant immune-mediated diseases on the disease course of inflammatory bowel disease
M. Attauabi1,2, M. Zhao1, F. Bendtsen1,2, J. Burisch1
1Gastrounit- Medical Division, Copenhagen University Hospital, Hvidovre, Denmark, 2Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
Background
Several studies have shown an association between inflammatory bowel diseases [IBD] and immune-mediated diseases [IMIDs], but data on the impact of co-occurring IMIDs on IBD course are inconsistent. The aim of this study was to investigate the impact of co-occurring IMIDs on IBD phenotype and disease course.
Methods
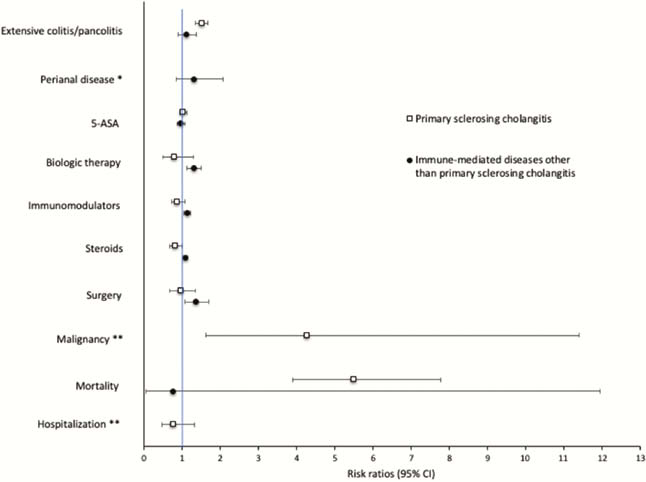
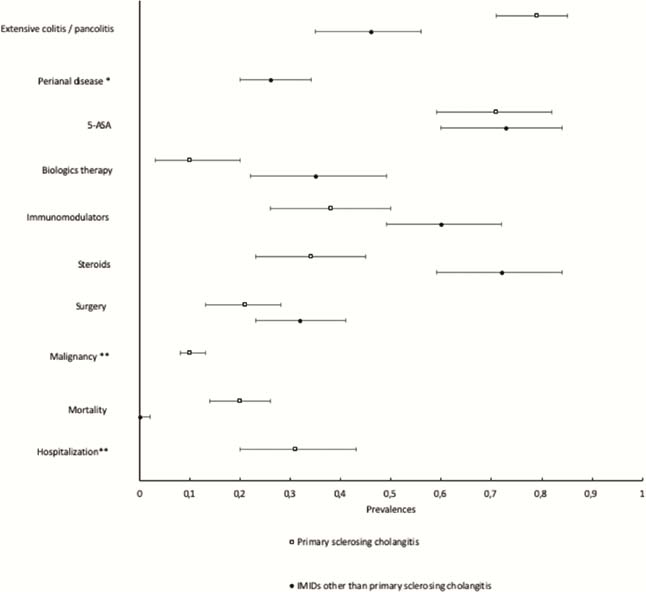
PubMed and EMBASE were searched from database inception through December 2018 and updated in October 2019 for studies reporting prevalences or odds, risks or hazard ratios of IBD-related disease outcomes in patients with and without co-existing IMIDs. Meta-analyses were performed to estimate summary prevalences and risks of the outcomes which included disease extension, IBD-related surgery and hospitalisation, malignancy, mortality and need of medication (biologic therapy, steroids and immunomodulators). IMIDs were stratified into primary sclerosing cholangitis [PSC] and ‘IMIDs other than PSC’.
Results
A total of 93 studies comprising 14,307 IBD patients with IMIDs and 3,409,914 IBD patients without IMIDs were included in the study. Summary risks and prevalences with 95% confidence intervals for each outcome are presented in figures 1 and 2, respectively. The following results are all significant (
Conclusion
This meta-analysis found that IBD patients with co-existing IMIDs have a different disease course than patients without concomitant IMIDs. This study emphasises the importance of multidisciplinary care of IBD and that physicians caring for IBD patients need to be aware of IMIDs as a prognostic factor.