
P273 Severity of colitis and clinical outcomes for patients admitted with acute UC in 2 large UK centres
Al Sulais, E.(1)*;Mukhtar, M.S.H.(2);Parkes, G.(3);Hart, A.(4);Raine , T.(1);
(1)Addenbrooke’s Hospital- University of Cambridge, Department of Gastroenterology, Cambridge, United Kingdom;(2)St. Mark’s Hospital and National Bowel Center, Gastroenterology- IBD Unit, London, United Kingdom;(3)Royal London Hospital, Department of Gastroenterology, London, United Kingdom;(4)St. Mark's Hospital and National Bowel Centre, Gastroenterology- IBD Unit, London, United Kingdom;
Background
Acute severe ulcerative colitis (ASUC) is a challenging complication of ulcerative colitis (UC) that can result in colectomy and even death. Management and recognition of the condition is based on criteria that have changed little since the 1950s (Truelove and Witts criteria). Patients may be admitted to hospital with acute colitis that does not meet criteria to be classed as severe. We hypothesised that such patients might be at risk of “over-management” if treated according to standard ASUC pathways.
Methods
We performed a retrospective review of inpatients managed for acute UC flares in two UK tertiary centres. We collected their baseline and outcome data. We assessed the proportion of patients meeting criteria for severe disease and compared outcomes between severe and non-severe groups.
Results
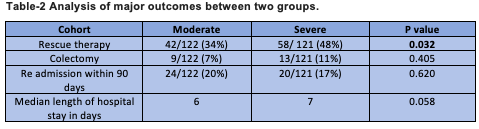
A total of 243 admissions for 200 unique patients were identified for analysis. A formal documentation of disease severity according to Truelove and Witts criteria was present in only 10/243 (4%). 121/243 (50%) met formal criteria for severe disease. Baseline demographic and disease characteristics were similar between patients with severe and non-severe disease (table-1). The use of rescue therapy was more common in the severe group (48% vs 34%, p=0.032). All other outcomes, including hospital length of stay, colectomy rates, and need for readmission were comparable (table-2).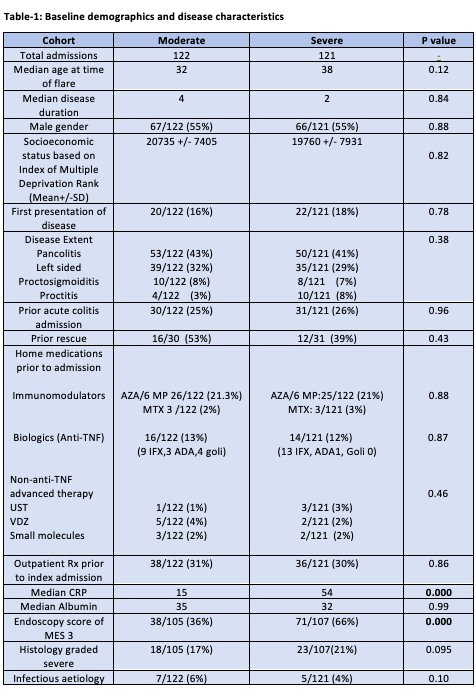
Conclusion
Patients admitted for acute colitis may frequently not meet criteria for severe disease. It is possible that earlier discharge or admission avoidance may be possible for this group. Baseline demographics do not appear to identify patients with less severe symptoms who nonetheless get admitted. Although rescue therapy was less common for non-severe patients, other outcomes were comparable, including length of stay and colectomy rates. There is a risk that once admitted, non-severe patients may receive management according to standard algorithms for severe disease, risking overtreatment for a subgroup of patients.