
P279 Early detection of mucinous adenocarcinoma within fistulating peri-anal Crohn’s disease
A. Corr1, L. Reza2, P. Lung1, I. Jenkins3, A. Antoniou3, A. Latchford4, A. Wilson4, N. Arebi4, D. Burling1, J. Warusavitarne3, O. Faiz3, S. Thomas-Gibson4, A. Hart4, P. Tozer2
1St Mark’s Hospital and Academic Institute, Department of Radiology, London, UK, 2St Mark’s Hospital and Academic Institute, Fistula Research Unit, London, UK, 3St Mark’s Hospital and Academic Institute, Colorectal surgery, London, UK, 4St Mark’s Hospital and Academic Institute, Department of Gastroenterology, London, UK
Background
The development of peri-anal fistula mucinous adenocarcinoma (MA) is a presumed rare but recognised event in patients with fistulating peri-anal Crohn’s disease. The true incidence is unknown, with a lack of robust registry data. Fistula mucinous cancers may evade early diagnosis, presenting with locally advanced intra-pelvic disease, necessitating debilitating and morbid exenterative surgery. Given the limitations of endoluminal assessment of this region in the context of an often extra-luminal disease process, MRI studies were reviewed in conjunction with EUA and endoscopic findings.
Methods
We performed a retrospective analysis of 8 cases of biopsy-proven mucinous adenocarcinoma (MA) that had developed within known Crohn’s related anal fistula. Serial MRI studies pre-dating the diagnosis of malignancy were reviewed in order to establish whether there are early predictive features of MA development within a fistula tract. Demographic, disease and surgical history were collected including the time of fistula diagnosis and histological confirmation of mucinous adenocarcinoma.
Results
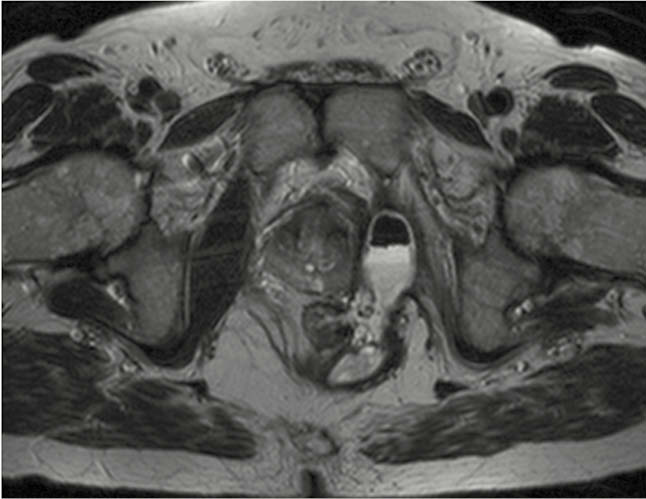
The median time to histological diagnosis of MA from the time of diagnosis of Crohn’s disease was 426 (96–480) months and from diagnosis of fistulating disease 66 (24–156) months. On review of sequential MRI fistula protocol studies, a characteristic ‘budding’ appearance within the T2 high signal ‘sepsis’/fistula tract is noted in all of our MA fistula cancer cases (Fig1 and 2). This finding pre-dates the histological diagnosis of MA by a median of 42(12–156) months. Weight loss was a presenting symptom in 4 of the 8 (50%) patients and all 8 patients reported a new significant peri-anal pain and high volume discharge which prompted reassessment and referral. Metastatic disease was not detected in any of the 8 cases. Potentially curative pelvic exenteration was possible in 7 patients.

Conclusion
Mucinous adenocarcinoma within this cohort often culminates in exenterative surgery by the time a diagnosis is made. There is an opportunity for early detection on MRI of the development of MA in an anal fistula by recognition of ‘budding’ within the tract. An earlier diagnosis may lessen the magnitude and morbidity of subsequent radical surgery following prolonged growth of these lesions. Long-standing Crohn’s anal fistula should be surveyed with MRI and any finding of ‘budding’ within the tract on T2 sequences should prompt urgent examination under anaesthetic and biopsy.