
P283 Patient-reported symptoms over a period of 14 days reliably predict endoscopic and histological disease activity in ulcerative colitis (UC)
A. Kormilitzin1, A.J. Walsh2, L. Matini2, R. Kantschuster2, M. Lepetyukh3, J. Wilson2, O. Brain2, R. Palmer2, T. Ambrose2, J. Satsangi2, S.P.L. Travis2
1Mathematical Institute, University of Oxford, Oxford, UK, 2Translational Gastroenterology Unit, Oxford University Hospitals NHS Foundation Trust, Oxford, UK, 3Oxford AHSN, Translational Gastroenterology Unit, Oxford, UK
Background
Disease activity assessment in UC is most accurately evaluated by endoscopy and biopsy, which often correlates poorly with current symptoms. We investigated whether a machine learning classification algorithm using patient-reported Simple Clinical Colitis Activity Index (SCCAI) over 14 days and signature features could reliably distinguish endoscopic and histopathologic activity from remission.
Methods
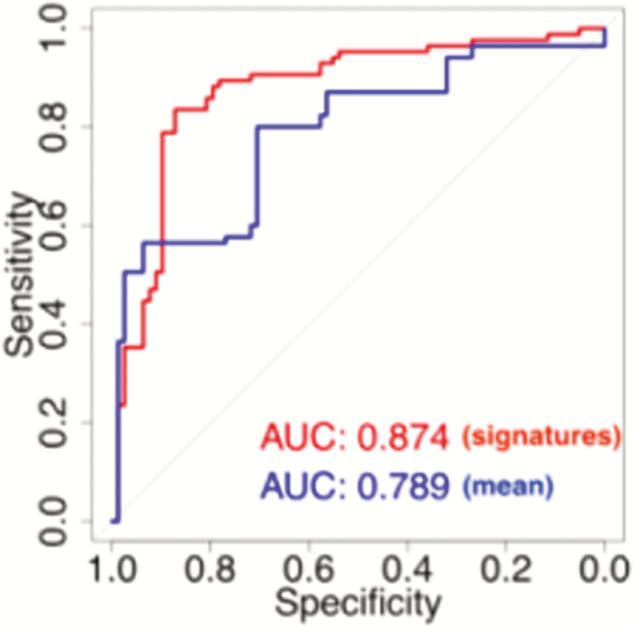
The TrueColours ulcerative colitis (UC) monitoring platform was used to collect symptoms (SCCAI, daily) and endoscopic/histopathological activity, as per the UCEIS and Nancy indices (twice in 6 months) in 233 patients. The longitudinal data may be seen as a trajectory. The signature is a collection of statistics which efficiently summarises the trajectory and serves as a non-parametric hierarchical method for longitudinal data representation. Signature features were used as input to the extreme gradient boosting classification algorithm to categorise subjects into remission or active disease groups. Remission: UCEIS ≤1 AND Nancy ≤1; Active disease: UCEIS ≥4 AND Nancy ≥2. The advanced signature-based approach was compared with a baseline model with manually constructed features (mean SCCAI score over 14 days preceding endoscopy). Cross-validation was used to report metrics, Table 1.
| AUC | 0.79 (0.72–0.86) | 0.87 (0.82–0.93) |
| Sensitivity | 0.87 (0.80–0.94) | 0.89 (0.83–0.95) |
| Specificity | 0.56 (0.46–0.68) | 0.78 (0.68–0.87) |
| Positive Predicted Value | 0.69 (0.63–0.75) | 0.82 (0.75–0.88) |
| Negative Predicted Value | 0.80 (0.71–0.89) | 0.87 (0.80–0.94) |
| Accuracy | 0.72 (0.66–0.79) | 0.84 (0.76–0.90) |
Results
Disease activity classification with signature features significantly outperformed mean-SCCAI based approach (AUC 0.87 vs. AUC 0.79 correspondingly,
Conclusion
Gradient boosting classification algorithm with signature features extracted from the longitudinal six-item symptoms of the SCCAI, reliably identified subjects with endoscopic and histopathological disease activity. The developed algorithm may be used with the TrueColours platform as a decision support tool.