
P335 Treatment strategies after mucosal healing (MH) in ulcerative colitis
A. Sitibondo1, A. Viola1, G. Costantino1, A. Centritto1, A. Belvedere1, V. Pisana1, A. Abbruzzese1, A. Alibrandi2, W. Fries1
1Inflammatory Bowel Disease Unit, Department of Clinical and Experimental Medicine, University of Messina, A.O.U. Policlinico ‘G. Martino’, Messina, Italy, 2Department of Economics, University of Messina, Messina, Italy
Background
MH and deep remission are the major therapeutic goals in the treatment of ulcerative colitis (UC), but the best therapeutic strategy after reaching MH in terms of maintenance or de-escalation is still poorly defined. This retrospective study aimed to evaluate the maintenance of remission in patients who maintained therapy vs. patients de-escalating treatment.
Methods
Data of patients with UC who reached mucosal healing were retrospectively investigated. Demographic data/gender, age), disease-related data (extension, duration, age at onset), together with data on smoking behaviour and on therapy after reaching MH were collected. MH was defined as an endoscopic Mayo score of 0. The primary endpoint was clinical relapse regardless of therapeutic regimen. The outcome of patients maintained on therapy was compared with patients who de-escalated therapy and to patients with mild disease maintained on mesalazine.
Results
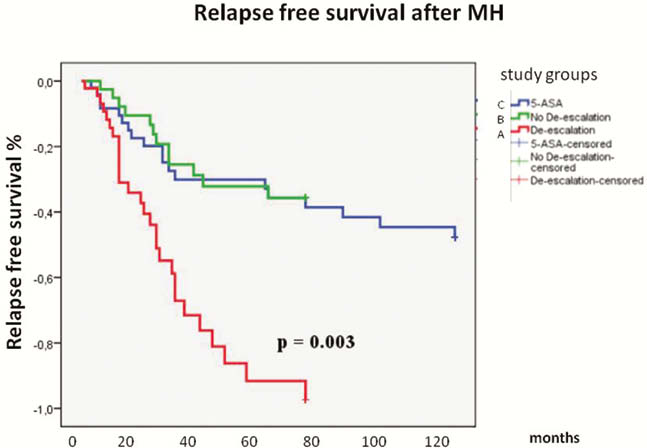
One hundred thirty-five patients with MH were followed for a mean time of 94 months (SD 57.2) and divided into 3 groups: group 1 (de-escalation; 45 patients), in which MH was reached with IMM or biologics and therapy was continued with only mesalazine, group 2 (no de-escalation; 40 patients) in which MH was reached with IMM or biologics, group 3 (only treatment with 5-ASA; 50 patients). In the 3 groups, disease relapse occurred in 62%, 30% and 38% respectively in a mean time of 22, 25 and 36 months. Patients who de-escalated therapy were more likely to relapse than patients who maintained initial treatment (
Conclusion
Maintaining treatment after MH is reached represents the best strategy to maintain remission. Patients on anti-TNFs were more likely to relapse after de-escalation. An evaluation on pharmacoeconomics seems to be advised in order to identify a more sustainable strategy.