
P341 Induction of response and remission: a network meta-analysis of induction studies comparing ontamalimab with other treatments for moderate-to-severe ulcerative colitis
A. Vickers1, A. Nag2, B. Devine3, B.E. Sands4, R. Panaccione5, L. Peyrin-Biroulet6, S. Danese7, S. Vermeire8, K.J. Gorelick9, M. Goetsch10, L. Hartley1
1Department of Data Analytics and Design Strategy, RTI Health Solutions, Manchester, UK, 2Outcomes Research and Epidemiology, Shire - a Takeda Company, Health Economics, Lexington, USA, 3School of Pharmacy, University of Washington, Seattle, USA, 4Dr Henry D. Janowitz Division of Gastroenterology, Icahn School of Medicine at Mount Sinai Medical Center, New York, USA, 5Division of Gastroenterology, University of Calgary, Calgary, Canada, 6Department of Gastroenterology, University Hospital of Nancy-Brabois, Vandœuvre-lès-Nancy, France, 7IBD Center, Humanitas University, Milan, Italy, 8Department of Gastroenterology, University Hospital Leuven, Leuven, Belgium, 9Zymo Consulting Group, Clinical Development, Newtown Square, USA, Clinical Development, 10Shire - a Takeda compa#ny, Zug, Switzerland
Background
Decisions regarding the treatment of ulcerative colitis (UC) should be based on appropriate, high-quality evidence. In the absence of head-to-head trials, network meta-analysis (NMA) can be used to compare the efficacy and safety of several treatments. We conducted an NMA to compare the efficacy of ontamalimab (anti-MAdCAM-1) using its phase 2 data, with all other biologics and novel small molecules for which induction study data on response and remission in patients with UC were available.
Methods
A systematic literature review was conducted in November 2017 to identify published randomised controlled trials of induction treatment in patients with moderate-to-severe UC. An NMA of the identified studies was performed using random-effects models and methods based on NICE guidance. Odds ratios and 95% credible intervals were calculated to describe the relative differences between all treatments and placebo in terms of efficacy in inducing response and remission. Results were generated for anti-TNF-naïve and -experienced populations.
Results
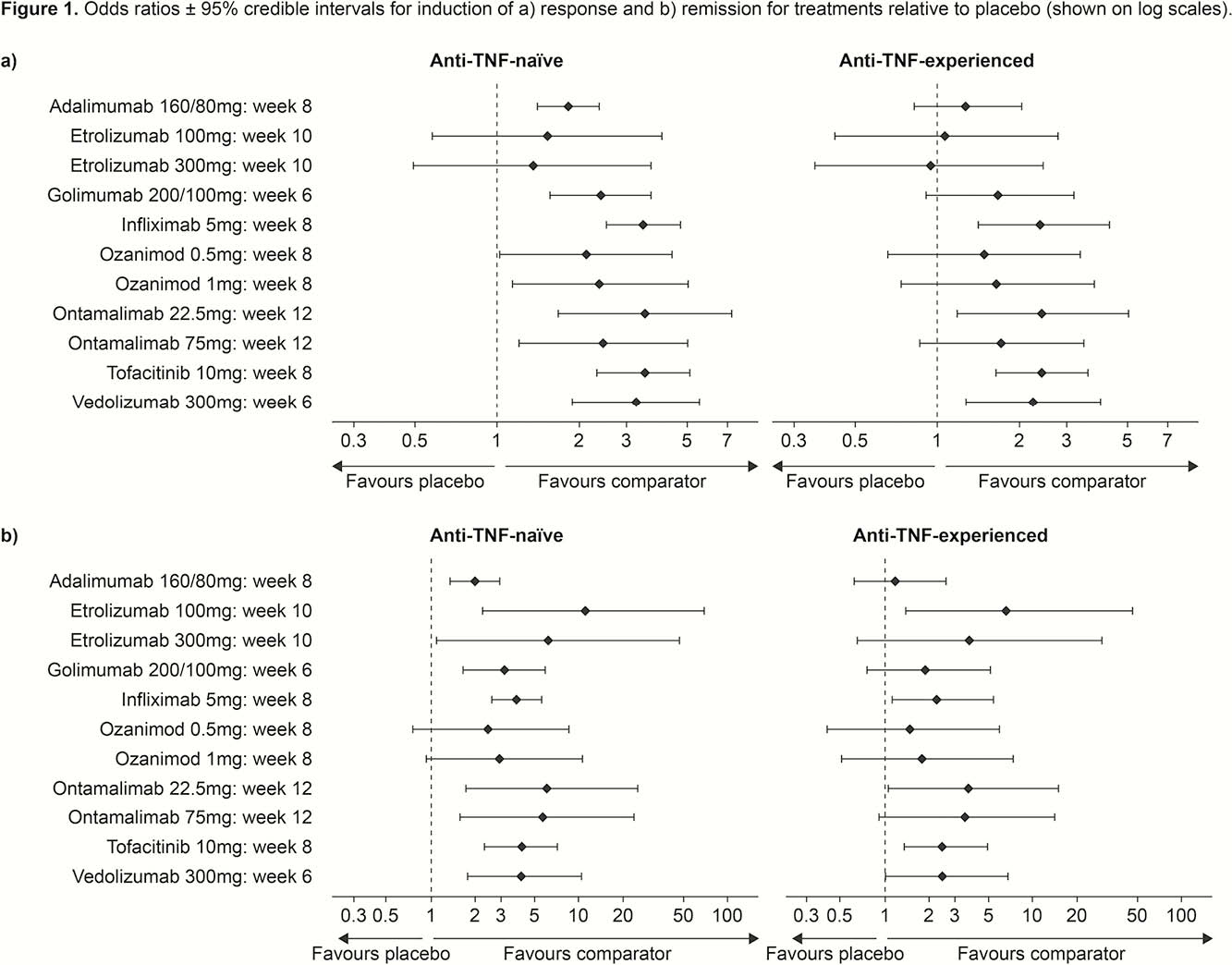
A total of 14 phase 2 and phase 3 induction studies of the following agents were included: adalimumab (160/80 mg), etrolizumab (100 mg and 300 mg), golimumab (200/100 mg), infliximab (5 mg), ontamalimab (22.5 mg and 75 mg), ozanimod (0.5 mg and 1 mg), tofacitinib (10 mg) and vedolizumab (300 mg). The definitions of response and remission used across trials were consistent. Between-study homogeneity was good and enabled pooling of results. Figure 1 shows odds ratios for induction of response and remission with treatments relative to placebo in anti-TNF-naïve and -experienced patients. All treatments, including ontamalimab, significantly differentiated from placebo in anti-TNF-naïve patients, with the exception of etrolizumab and ozanimod for response and remission, respectively. Tofacitinib (
Conclusion
This study suggests ontamalimab and most other treatments induce response and remission better than placebo. Although conducted before any large-scale head-to-head trials of these drugs, the study suggests a few treatments could be superior to adalimumab in terms of efficacy. However, varying endpoint timings, the combination of phase 2 and 3 data, and lack of control for placebo response could underscore large variances in the data and preclude firm conclusions being drawn.