
P360 The correlation between ophthalmological posterior segment findings and disease severity in patients with inflammatory bowel disease
Mitrovic, M.(1);Jeremić, M.(2);Zlatković, D.(1);Pantelić, M.(1);Vrinić-Kalem, D.(1);
(1)University Medical Center Zvezdara, Department of Gastroenterology, Belgrade, Serbia;(2)Eye Clinic- Clinical Center Serbia, Eye Clinic, Belgrade, Serbia;
Background
Inflammatory bowel disease (IBD) is often associated with ophatlmological complications, such as blepharitis, conjunctivitis, episcleritis and iridociclitis. Although present in approximately quarter of all IBD patients, ophthalmological posterior segment findings are often overseen and possibly related to disease activity.
Methods
A total of 136 patients, with previous IBD, underwent a complete ophthalmological examination, including fundus photography and optical coherence tomography/angiography (OCT/OCTA) using Optovue Avanti XR HD-OCT. The retinal foveolar avascular zone (FAZ) and choroidal thickness was measured using AngioPlex OCTA software. IBD activity was evaluated using adapted Mayo score and Crohn's disease activity index (CDAI), for ulcerative colitis (UC) and Crohn's disease (CD), respectively, as well as faecal calprotectin and serum C-reactive protein levels. UC remission based on the modified Mayo score was defined as stool frequency sub-score 0 to 1, rectal bleeding sub-score of 0, and endoscopy sub-score 0 to 1. CD remission was defined with CDAI score bellow 150. Patients with recent ophthalmological surgery, refractive errors greater than +3 or -3, as well as patients with retinopathies were excluded from analysis.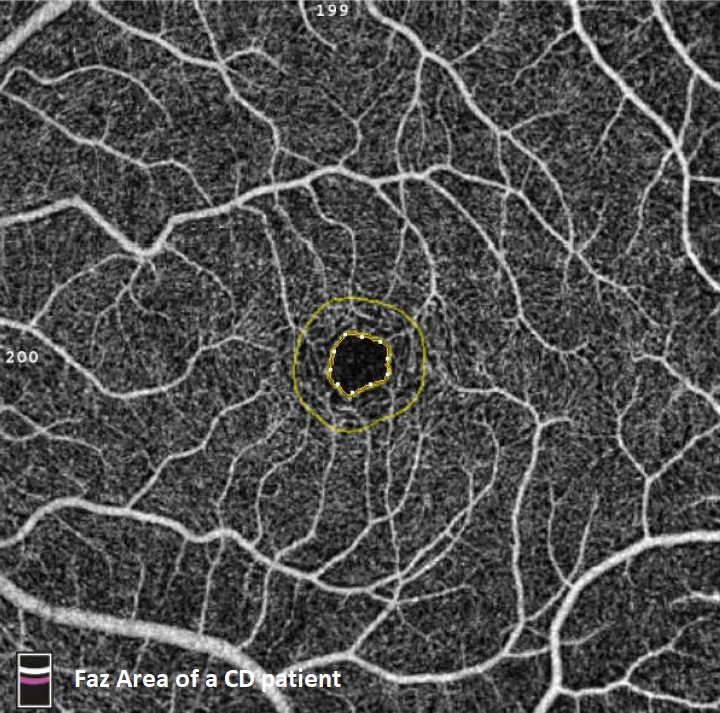
Results
We performed a cross-sectional study of 272 eyes of 136 IBD patients (91 UC and 45 CD) average age 45 years, of which 87 females. A total of 37 patients (27.2%), of which 18 UC and 19 CD patients, were defined as having an active disease. The most prevalent fundoscopic finding was vascular tortuosity, observed in 47 eyes (17.2%). The difference between choroidal thickness between UC and CD patients was not observed (308±35µm vs 314±29µm, p=0.32), as well as the FAZ difference (0.32 vs 0.33 mm2, p=0.21). On the other hand, if we take in count only patients with active disease, the FAZ area of CD patients was significantly greater in comparison to UC patients (0.31 vs 0.34 mm2, p=0.028). Correlation study showed significant correlation between choroidal thickness and CDAI (Rho 0.448, p=0.036).
Conclusion
The choroidal thickness and FAZ area are ophthalmological parameters that could be easily obtained using OCTA and may be taken in count as possible non-invasive markers of disease severity, especially in CD patients.