P367 Significant impact on health care utilization upon implementation of an electronic IBD care management program.
Koppelman, L.(1)*;Roozemoind, S.(1);Cornelissen, L.(2);Hommes, D.(2);Voorneveld, P.(1);Maljaars, J.(1);Kubben, F.(3);Verweij, E.(3);van der Meulen - de Jong, A.(1);
(1)Leiden University Medical Centre, gastroenterology, Leiden, The Netherlands;(2)DEARhealth BV, DEARhealth, Amsterdam, The Netherlands;(3)Maasstad Ziekenhuis, gastroenterology, Rotterdam, The Netherlands;
Background
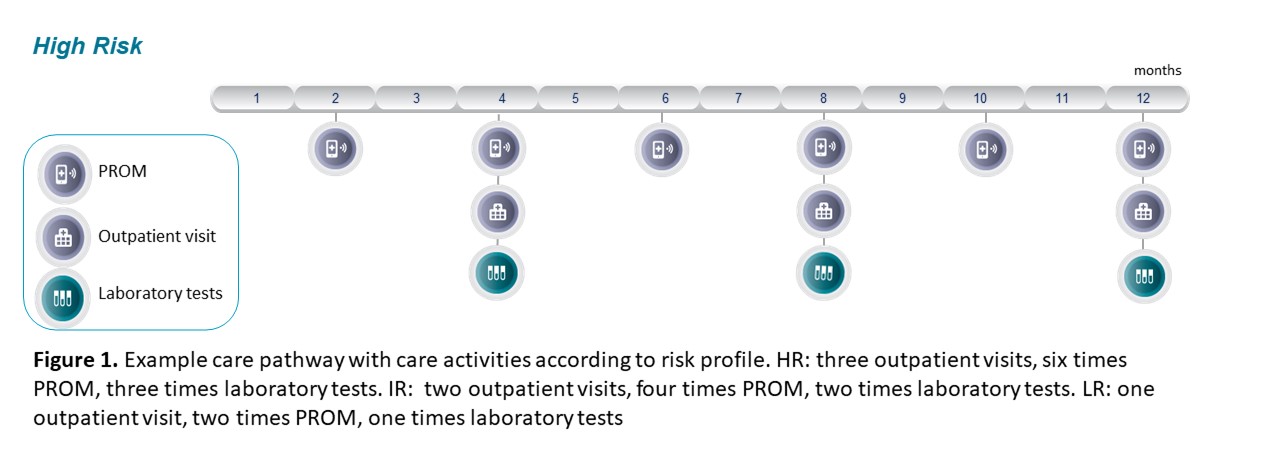
The management of Inflammatory Bowel Diseases (IBD) remains to be a significant challenge because of its unpredictable clinical course and high associated costs. Recently, we implemented an electronic IBD care management program, provided by DEARhealth BV, which offers care-pathways that configurate according to individual IBD risk profiles, called THINK. High-risk (HR) IBD patients (current biochemical disease activity) will receive more intense monitoring and provider interactions compared to Low-risk (LR) (>3 years in remission) and Intermediate-risk (IR) (other patients) individuals (figure 1). In this project, before implementation of THINK, we aimed to assess whether 1. Current healthcare utilisation (HCU) (consultations, lab tests, calprotectin) differs between risk groups and 2, what the effect of implementing THINK would be on HCU (focused on consultations and laboratory tests) in a retrospective-analysed population.
Methods
161 consecutive IBD patients in hospital A, categorized in either the HR or IR group, were studied prospectively during 1 year before implementation of THINK. HCU was captured using an electronical medical record (EMR) and included consultations, blood tests and calprotectin. Furthermore, HCU in the years 2018-2019 in the IBD population of hospital B was studied (extraction of EMR). This historical data was compared to the THINK care path (see figure 1) when optimal implemented. The analysis focused on the activities present in de THINK care pathway (consultations and laboratory tests) to uncover the potential of the electronic IBD care management program.
Results
Baseline characteristics for hospital A cohort (N=161) are summed in Table 1. We followed 102 patients (60 Crohn) in the IR group and 59 patients in the HR group (29 Crohn). As expected, significant more HCU was present in the HR group (table 2). In hospital B, the utilization impact assessment was performed in the IBD cohort of 543 Crohn and 495 colitis patients. A difference in clinic consults was observed of -52,7% (HR), -53.5% (IR) and -29,3% (LR). The difference in laboratory tests utilization was found -54,0% (HR), -27.8% (IR) and -3,1% (LR).
Conclusion
Our initial experiences with a novel IBD management program demonstrated the feasibility of accurate remote disease activity monitoring and significant impact on utilization patterns due to the risk-based care pathway configurations. However, the analysis shows the ideal fictive situation when using standardized care pathways which cannot fully be considered the real-time situation. In this analysis no unexpected events are included. Future research should investigate the realization of these predictions.