
P372 Effects of filgotinib on anaemia, thrombocytopenia and leukopenia: Phase 3 study results in patients with active rheumatoid arthritis and prior inadequate response/intolerance to biological DMARDs
R. Besuyen1, M. Genovese2, K. de Vlam3, J.E. Gottenberg4, K. Kalunian5, B. Bartok6, Y. Tan7, Y. Guo8, C. Tasset1, J. Sundy9, D. Walker10, T. Takeuchi11
1Galapagos NV, Clinical Development, Mechelen, Belgium, 2Division of Immunology and Rheumatology, Stanford University, Palo Alto, CA, USA, 3Department of Rheumatology, Universitair Ziekenhuis Leuven, Leuven, Belgium, 4Department of Rheumatology, Strasbourg University Hospital, Strasbourg, France, 5Division of Rheumatology- Allergy and Immunology, University of California, San Diego, CA, USA, 6Medical Affairs, Gilead Sciences Inc., Foster City, CA, USA, 7Clinical Development, Gilead Sciences Inc., Foster City, CA, USA, 8Biostatistics, Gilead Sciences Inc., Foster City, CA, USA, 9Clinical Research, Gilead Sciences Inc., Foster City, CA, USA, 10Department of Rheumatology, Northumbria Healthcare, Northumbria, UK, 11Division of Rheumatology and Clinical Immunology, Keio University School of Medicine, Tokyo, Japan
Background
Anaemia, thrombocytopenia and leukopenia in rheumatoid arthritis (RA) patients treated with non-Janus Kinase 1 (JAK1) selective inhibitors may be due to inhibition of haematopoietic growth factors signalling through JAK2. Therefore, we investigated anaemia, thrombocytopenia and leukopenia in patients with active RA with prior inadequate response/intolerance to biologic disease-modifying anti-rheumatic drugs (bDMARDs) treated with filgotinib (FIL), a selective JAK1 inhibitor (FINCH-2; NCT02873936).
Methods
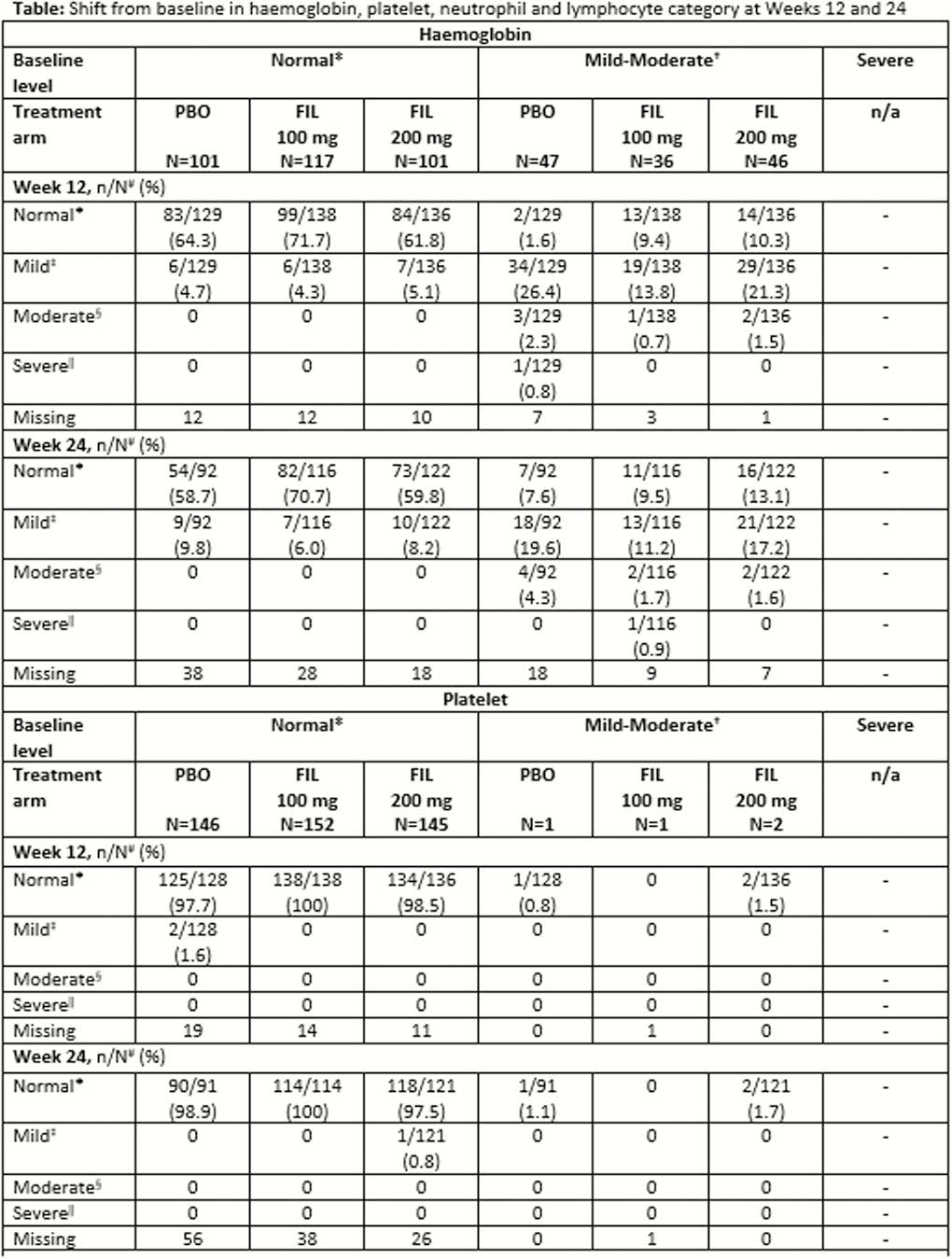
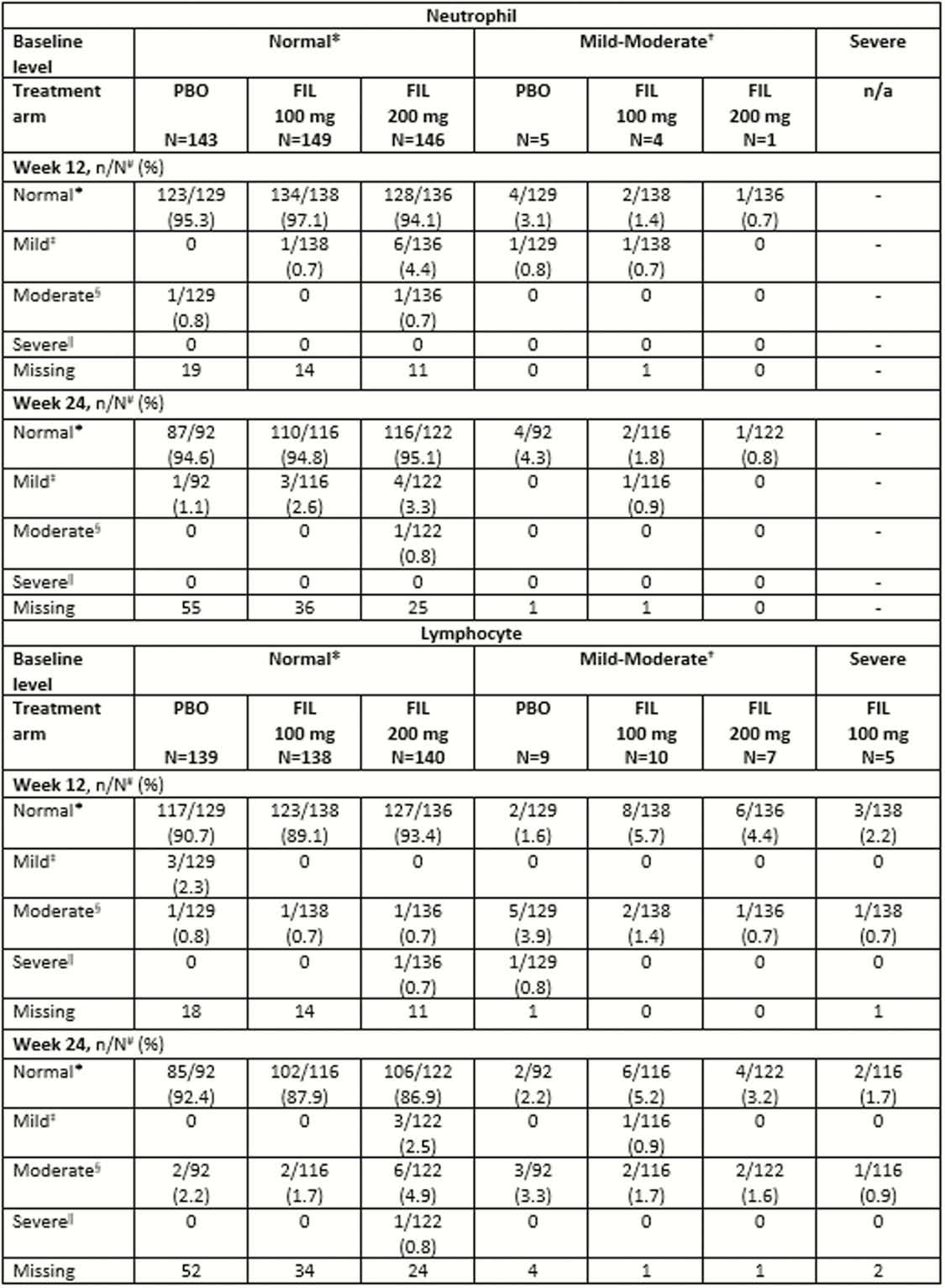
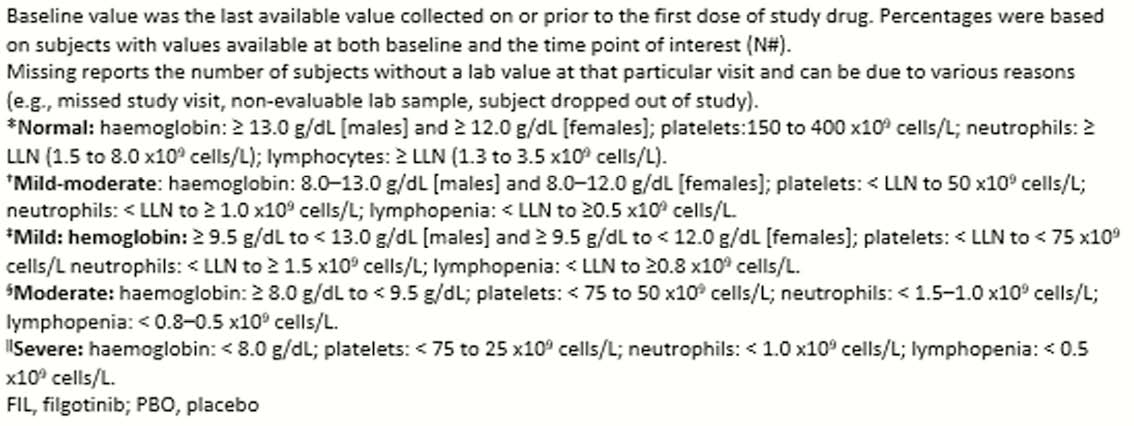
In the randomised, double-blind, placebo-controlled Phase 3 FINCH-2 trial, patients were randomised 1:1:1 to oral FIL 200 mg, 100 mg, or placebo (PBO) once daily plus conventional synthetic DMARDs for 24 weeks. In this subgroup analysis, we assessed shifts from baseline (BL) in haemoglobin (hgb), platelets (plt), neutrophils and lymphocytes.
Results
A total of 448 patients were treated; FIL 200 mg,
Conclusion
In this subgroup analysis, most patients with normal hgb, plt, lymphocyte and neutrophil at BL maintained them over 24 weeks of FIL treatment. Of the patients with mild–moderately low hgb at BL, >9% shifted towards normalisation. Similar patterns of improvement were observed for plt, lymphocyte and neutrophil counts. These results suggest that FIL does not increase the incidence of anaemia, thrombocytopenia or leukopenia in patients who entered the study with active RA despite prior bDMARDs.