
P387 Real-world clinical outcomes of biologic-naïve non-complicated Crohn’s disease patients treated with vedolizumab: Results from the EVOLVE study
A. Yarur1, G.J. Mantzaris2, U. Kopylov3, M. Bassel4, N. Brett4, H. Kim5, C. Lopez6, S. Saha7, C. Kifnidi8, C. Agboton9, S. Adsul9, D. Demuth10, M. Luo11, S. Wang11, B. Bressler12
1Gastroenterology, Medical College of Wisconsin, Milwaukee, USA, 2Gastroenterology, Evangelismos Hospital, Athens, Greece, 3Sheba Medical Center, Gastroenterology, Tel Aviv, Israel, 4Evidera, Real-World Evidence, Montreal, Canada, 5Evidera, Data Analytics, Waltham, USA, 6Takeda Pharmaceuticals USA Inc., Medical Affairs, Deerfield, USA, 7Takeda Canada Inc., Medical Affairs, Oakville, Canada, 8Takeda Hellas S.A., Medical Affairs, Athens, Greece, 9Takeda Pharmaceuticals International AG, Global Medical Affairs, Zurich, Switzerland, 10Takeda Pharmaceuticals International, Evidence Generation and Publications, Singapore, Singapore, 11Takeda Pharmaceuticals International, Global Outcomes Research, Boston, USA, 12St. Paul’s Hospital, Gastroenterology, Vancouver, Canada
Background
Crohn’s disease (CD) can lead to complications that impact treatment (Tx) decisions and its clinical effectiveness. The objective of this analysis was to compare clinical effectiveness outcomes of CD patients treated with first-line biologic vedolizumab (VDZ) who did not have a complicated disease phenotype (non-complicated) to VDZ patients who had complications (complex disease).
Methods
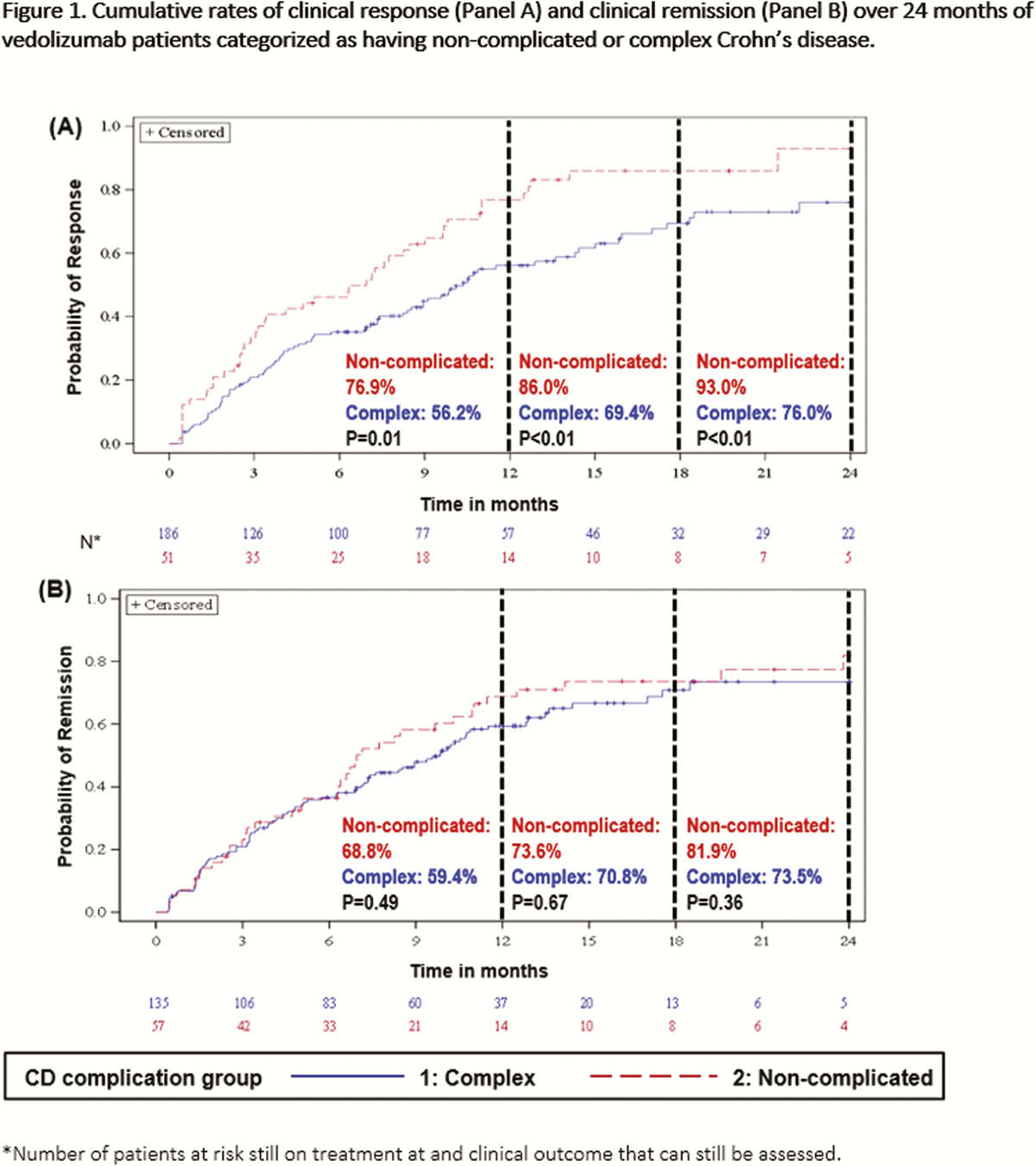
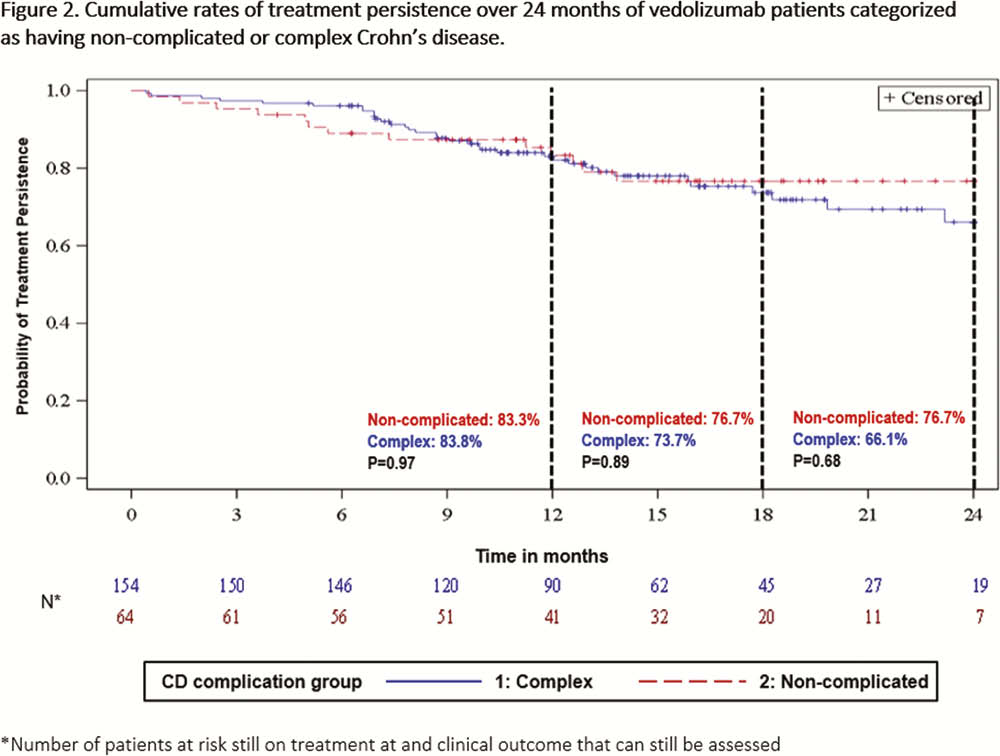
This was a retrospective real-world cohort study of biologic-naïve CD patients (≥18 years old) in Canada, Greece and the USA who initiated VDZ Tx between May 2014 and March 2018. Data were collected from Tx initiation to the earliest of chart abstraction date or death. The non-complicated CD was defined as patients who had mild or moderate disease severity and no active fistula at Tx initiation, had no prior CD-related surgeries since diagnosis and no CD-related hospitalisations within 12 months prior to Tx initiation. The complex disease cohort encompassed all other CD patients. Cumulative rates of clinical effectiveness outcomes over 24 months (Tx persistence, clinical response and clinical remission) were estimated using the Kaplan–Meier method. Using pre-defined hierarchical algorithms, clinical response and clinical remission were assessed from standard disease measures reported in the medical records.
Results
This analysis included 218 CD patients treated with VDZ (non-complicated: 64 (29.3%); complex: 154 (70.6%) from 37 sites. Mean (SD) age at Tx initiation: non-complicated, 46.2 (15.8); complex, 54.0 (16.7); male: non-complicated, 45.3%; complex, 55.2%. Cumulative rates of clinical response were significantly greater in non-complicated than complex disease patients over 24 months (non-complicated: 93.0%, complex: 76.0%,
Conclusion
A high proportion of patients (70%) had a complex disease when VDZ Tx was initiated but those with non-complicated phenotype had a higher response rate. To help guide physicians in positioning the optimal Tx for biologic-naïve CD patients, it is important to identify the sub-group of patients who can most benefit from VDZ Tx. The results of this real-world study suggest that the biologic-naïve, non-complicated CD patients benefit more from VDZ treatment compared with those with disease complications.