
P405 Primary non-response and loss-of-response to first-line biological therapies are more common in patients with Ulcerative Colitis than Crohn’s Disease – preliminary results from the Danish IBD Biobank Project
Zhao, M.(1);Larsen, L.(2);Dige, A.(3);Hvas, C.L.(3);Poulsen, A.(4);Christiansen, D.(4);Attauabi, M.(1,5);Lo, B.(1);Wewer, M.(1,6);Ovesen, P.D.(6);Petersen, A.M.(1,7);Bendtsen, F.(1);Seidelin, J.B.(5);Burisch, J.(1,4);
(1)Hvidovre University Hospital, Gastro Unit- Medical Division, Hvidovre, Denmark;(2)Aalborg University Hospital, Dept. of Gastroenterology and Hepatology, Aalborg, Denmark;(3)Aarhus University Hospital, Dept. of Hepatology and Gastroenterology, Aarhus, Denmark;(4)Bispebjerg Hospital, Digestive Disease Centre, Copenhagen, Denmark;(5)Herlev University Hospital, The Gastro Unit- Medical Division, Hvidovre, Denmark;(6)University of Copenhagen, Faculty of Health and Medical Sciences, Copenhagen, Denmark;(7)Hvidovre University Hospital, Dept. of Clinical Microbiology, Hvidovre, Denmark;
Background
The use and cost of biological treatment in patients with inflammatory bowel diseases (IBD) continue to rise. Meanwhile, rates of primary non-response (PNR) and loss of response (LOR) are high. We aimed to investigate predictors of PNR and LOR in a real-world cohort of bio-naïve IBD patients.
Methods
This study included 488 adult patients with IBD (52% UC, 47% CD, 1% IBDU) who initiated and completed induction therapy with a biological drug from May 2019 – Oct 2021 at five university hospitals covering 2.1 M inhabitants. Clinical response to induction therapy was defined as a decrease at week 14 in the Simple Clinical Colitis Activity Index (SCCAI)>1 in UC and a decrease in Harvey Bradshaw Index (HBI)>3 in CD patients. Clinical remission was defined as SCCAI<3 in UC and HBI<5 in CD. PNR was defined as lack of response or IBD surgery during the induction period. LOR was defined as need for systemic steroids, drug switch or IBD surgery during maintenance therapy. Multivariable logistic regression and COX-regression analyses were performed to assess predictors of outcomes.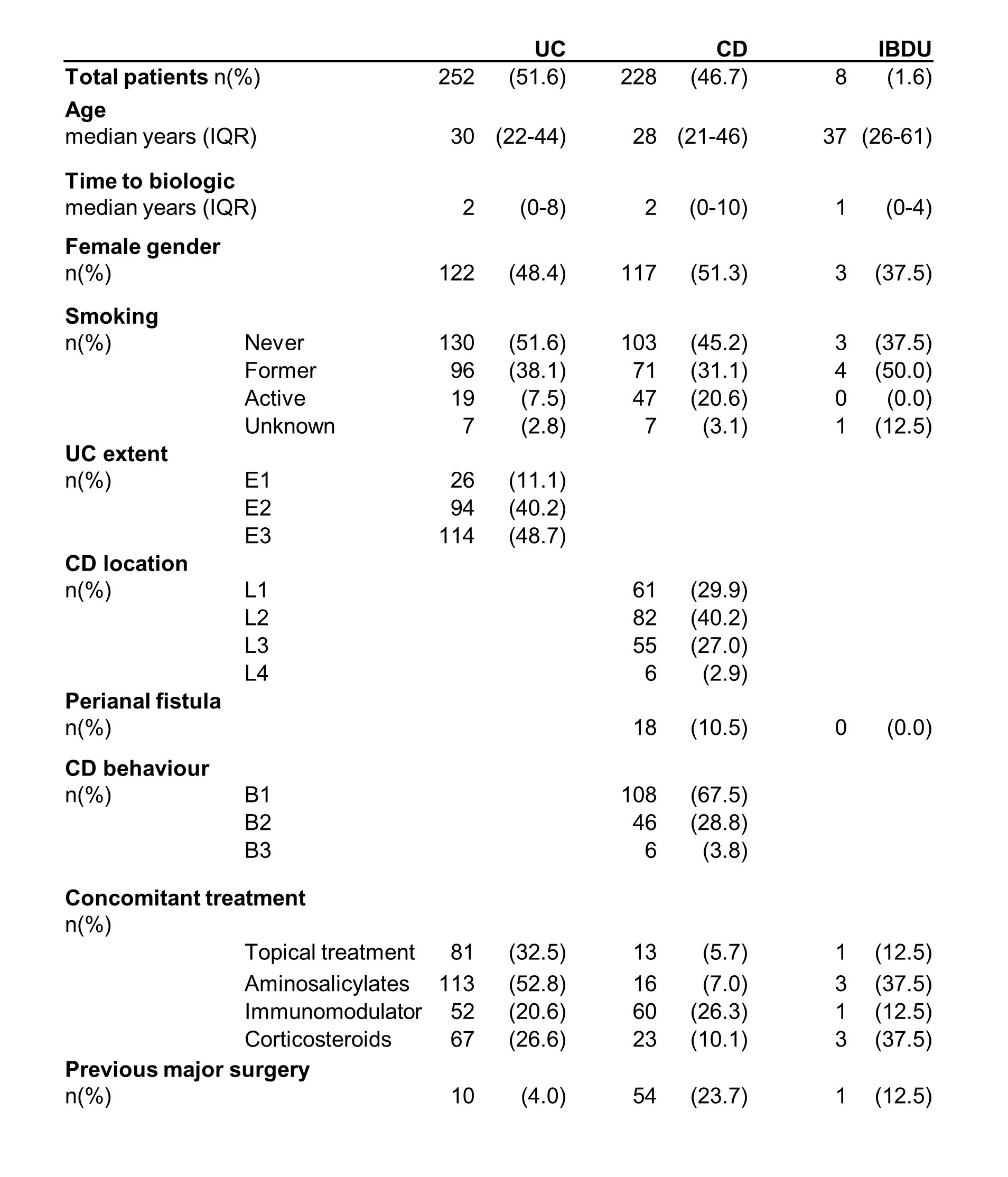
Results
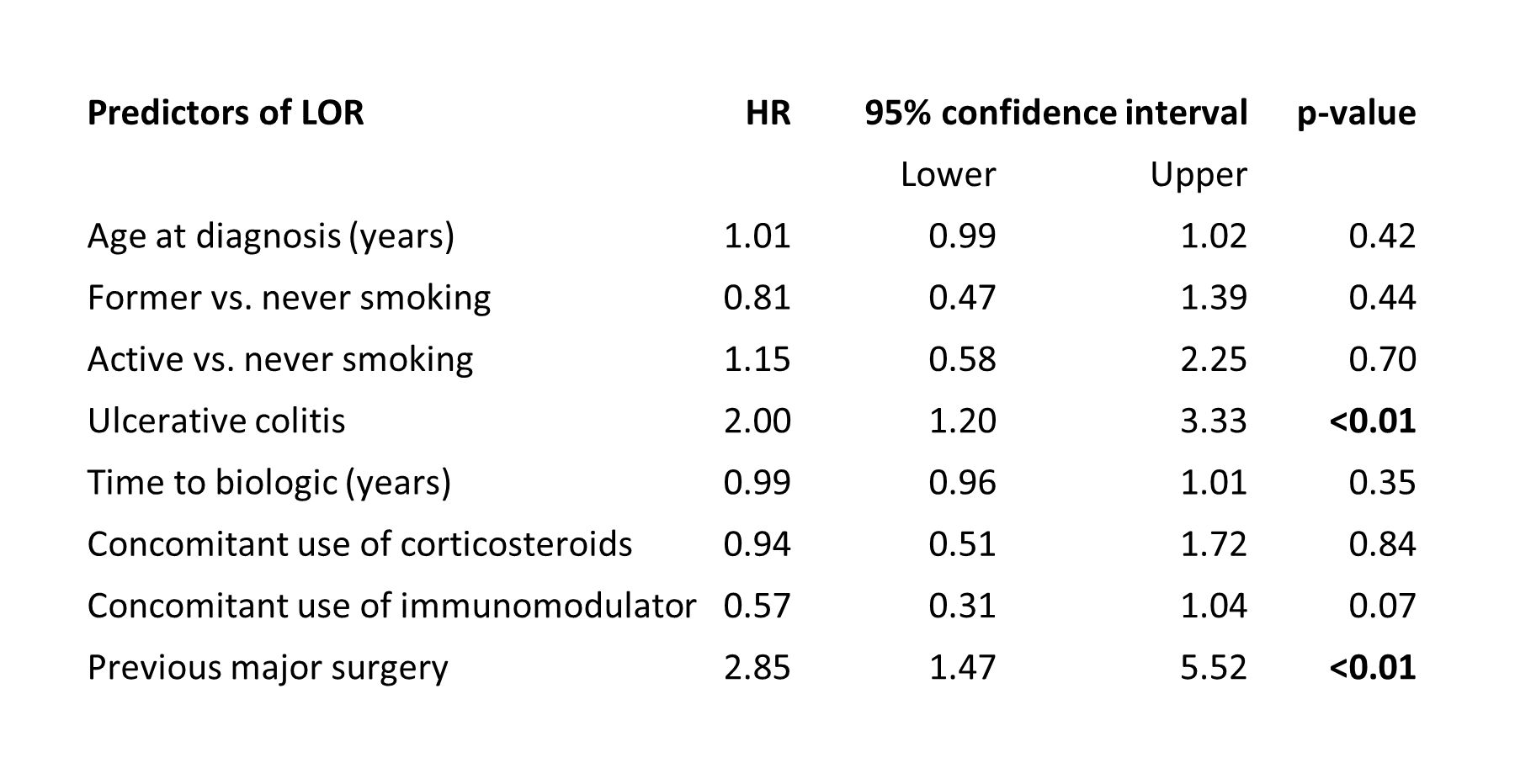
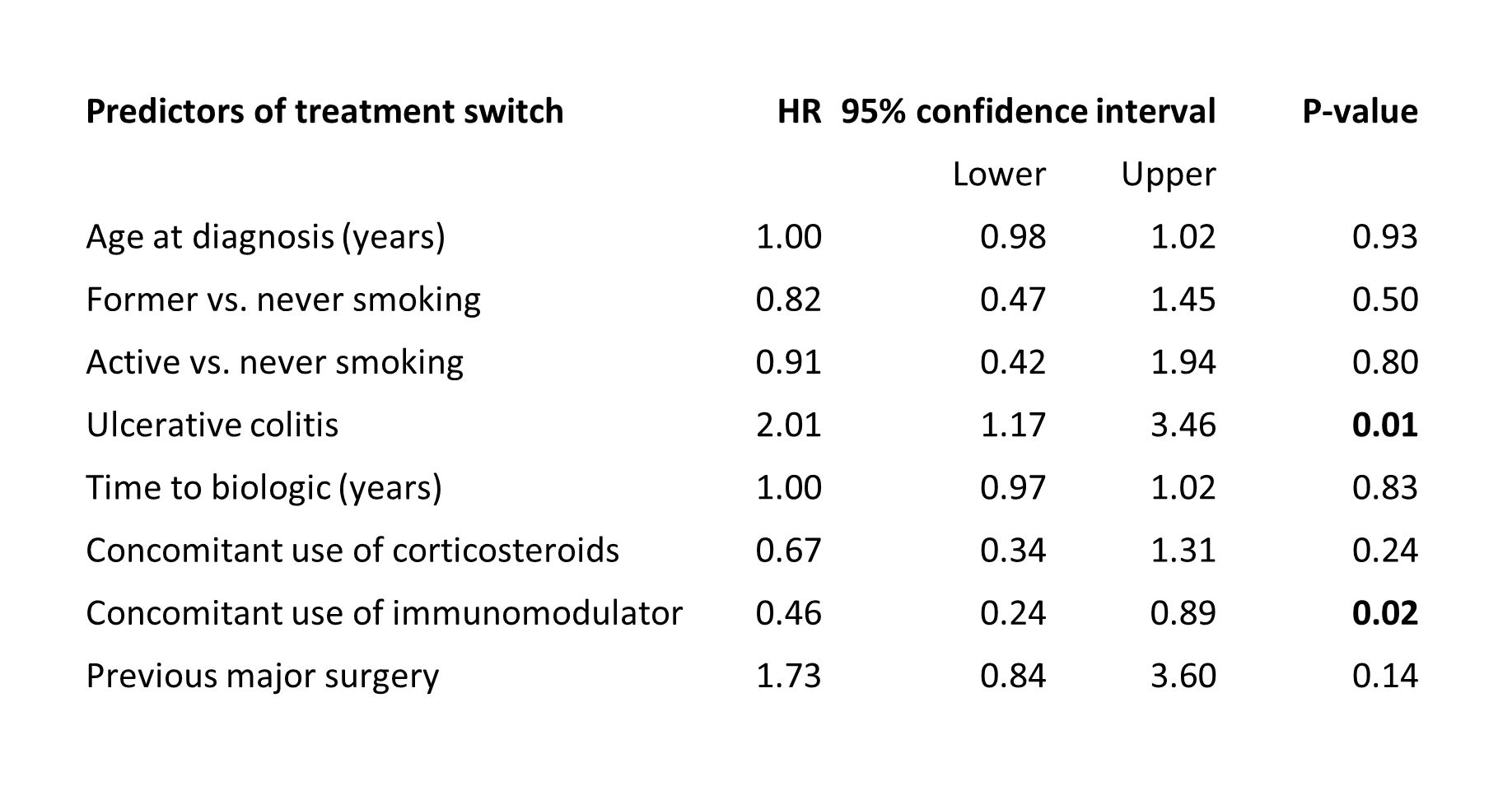
Biological treatment was initiated after a median of two years (IQR 0-9.Table 1). Most patients were treated with infliximab(97%) followed by adalimumab(2%) and vedolizumab (1%). Luminal activity was the most common indication(67%) followed by acute severe UC(17%) and need for post-operative prophylaxis(7%). Treatment was discontinued in 27(6%) patients due to other reasons than PNR during induction therapy. PNR occurred in 95(30%) of 314 patients with available scores and was higher in UC patients (OR 2.19,95%CI 1.19-4.05,p=0.01.Table 2), but lower in those who were former smokers (OR 0.51,95%CI 0.27-0.95,p=0.03). Clinical remission was achieved in 234(52%) patients and lower in those with UC (OR 0.48,95%CI 0.32-0.74,p<0.01) or previous major surgery (OR 0.48,95%CI 0.25-0.92,p=0.03). LOR occurred in 82(21%) of 395 patients who received maintenance therapy. LOR rate was higher in patients with UC (HR 2.00,95%CI 1.20-3.33,p<0.01) and previous major surgery (HR 2.85,95%CI 1.47-5.52,p<0.01.Table 3). UC was associated with a higher risk of drug discontinuation (HR 1.85,95%CI 1.20-2.85,p<0.01) and switch (HR 2.01,95%CI 1.17-3.46,p=0.01) whereas concomitant use of immunomodulator (IM) lowered the risk of both (HR 0.47,95%CI 0.27-0.81,p<0.01 and HR 0.46,95%CI 0.24-0.89,p=0.02.Table 4).
Conclusion
PNR occurred in one of four patients and LOR in one-fifth. Both PNR and LOR rates were higher in patients with UC. During maintenance therapy, UC patients had a higher risk of drug discontinuation and switch whereas concomitant use of IM decreased the risk of both.
Funding: unrestricted grant from Takeda A/S, Louis-Hansen Fonden and public fund hosted by Hvidovre Hospital.