
P485 Switching infliximab biosimilar: No adverse impact on inflammatory bowel disease control or drug levels with the first or second switch
R. Luber1, R. O’Neill2, S. Singh2, Z. Arkir3, P. Irving1
1Department of Gastroenterology, Guy’s and St Thomas’ NHS Foundation Trust, London, UK, 2Department of Pharmacy, Guy’s and St Thomas’ NHS Foundation Trust, London, UK, 3Guy’s and St Thomas’ NHS Foundation Trust, Viapath, London, UK
Background
Biological medicines account for a significant cost to healthcare systems. With the advent of anti-tumour necrosis factor biosimilars, switching from originator to biosimilar has enabled cost saving in inflammatory bowel disease (IBD) without compromising disease control. However, with more biosimilars entering the market, the effect on IBD activity and pharmacokinetics (PK) of a second switch to another biosimilar is uncertain. This study aims to assess the effect on disease activity and drug levels associated with switching from infliximab (IFX) biosimilar Remsima® (Celltrion, Hungary) to another biosimilar, Flixabi® (Samsung Bioepis, The Netherlands), and to compare those switching for the first and second time.
Methods
All IBD patients on IFX biosimilar Remsima® were prospectively followed during their switch to Flixabi® in a single centre. Baseline data including C-reactive protein (CRP), trough IFX level, and clinical disease activity indices were collected; Harvey Bradshaw Index for Crohn’s disease (CD) and Simple Clinical Colitis Activity Index for ulcerative colitis (UC). These indices were repeated after at least two infusions of Flixabi®.
Results
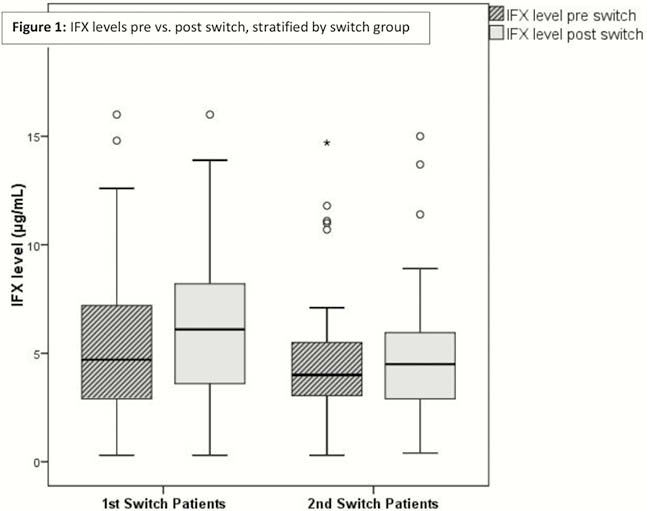
221 patients (179 CD, 42 UC) on stable IFX treatment were included in the study. 174 (79%) were on a concomitant immunomodulator. 5 (2%) patients ceased IFX prior to follow-up due to sustained remission, and 3 (1%) patients discontinued due to factors not directly related to drug or disease. 112 patients had PK analysis performed pre and post switch. An increase in IFX trough level was observed after switching IFX biosimilars; baseline median (IQR) trough level of 4.5µg/ml (2.9–6.3) compared with post switch of 5.1µg/ml (3.4–7.0) (
Conclusion
In a cohort of IBD patients switching to a new IFX biosimilar either for the first or second time, an increase in IFX level was observed with no impact on clinical and biochemical disease activity indices. Switching IFX biosimilars in IBD appears safe in the short term with respect to maintaining drug pharmacokinetic profile and disease control whether switching for the first or second time.