
P505 Different failure rates after non-medical switching of 744 patients from adalimumab originator to 2 different adalimumab biosimilars at Cambridge University Hospitals, UK: real-world experience
D. Rosembert1, A. Malaviya2, J. How2, J. Tomlison3, F. Toh3, M. Roe1, A. Nightingale4, C. Garcia-Sueiro4, P. Herbert4, D. Jadon2, P. Norris3, J. Thomas3, J. Magsino4, A. Negoescu2, T. Raine4
1Department of Pharmacy, Cambridge University Hospitals, Cambridge, UK, 2Department of Rheumatology, Cambridge University Hospitals, Cambridge, UK, 3Department of Dermatology, Cambridge University Hospitals, Cambridge, UK, 4Department of Gastroenterology, Cambridge University Hospitals, Cambridge, UK
Background
Biosimilar adalimumab became available in the UK in October 2018, with payers introducing a series of measures to drive the adoption of the ‘best value’ adalimumab.1 Consideration of value should include risk of loss of efficacy and adverse reactions, which might drive further biologic switches or ‘reverse switches’ to originator. Managing potential ‘nocebo effect’ requires high levels of patient engagement, whilst the presence or absence of citrate buffer may affect patient-reported discomfort, hence patient treatment perceptions.
Methods
Patients were switched to 2 different biosimilar adalimumabs, one buffered with citrate (ADA1) and one in a citrate-free buffer (ADA2). The choice of adalimumab biosimilar was made for clinical and economic reasons. Patients were informed of the switch to either ADA1 or ADA2 in advance via letter and at clinic visits. Patients who reported problems after switching were reviewed.
Results
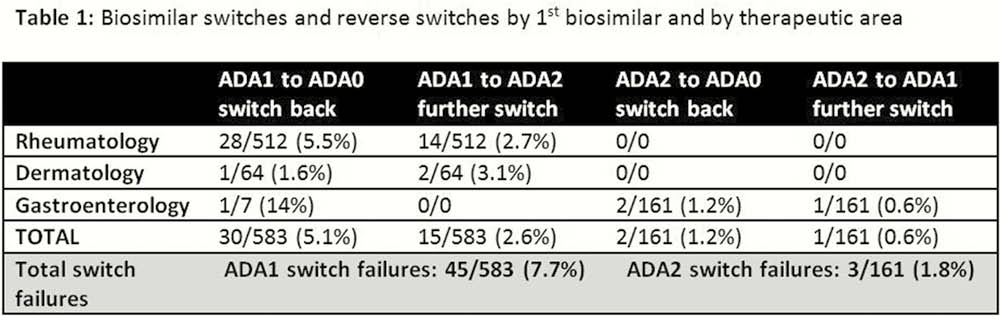
A total of 744 patients were switched from originator adalimumab (ADA0) to ADA1 or ADA2. Rheumatology and dermatology patients were switched to ADA1, whilst gastroenterology patients were switched to ADA2, except for those with a latex allergy, where ADA1 was used (or ADA2 in a latex-free syringe). A total of 49 (6.6%) patients reported problems and a further switch of drug was judged necessary in 48 (Table 1). Switch failure was significantly more likely with ADA1 than ADA2 (7.7% vs. 1.8%;
Conclusion
In the context of an effective patient communication strategy, adalimumab biosimilar switching was associated with overall low rates of patient-reported problems in a large cohort. Despite an identical communication strategy, significantly higher rates of injection site problems and disease flares were seen between 2 different biosimilars, reflected in a higher need for further switches. These differences may impact the cost-effectiveness of any chosen strategy.
NHSE Biosimilar medicines https://www.england.nhs.uk/medicines/biosimilar-medicines/ cited 14.11.2019