
P514 Optimising response to infliximab in the management of perianal Crohn’s disease
SHAH , R.(1);Anandbaskaran , S.(1);Hart , A.(1);Tozer , P.(1);
(1)St Mark's Hospital- London North West Hospitals NHS Trust, Inflammatory Bowel Disease, London, United Kingdom;
Background
Perianal Crohn’s Disease (PCD) remains a refractory phenotype of Crohn’s Disease (CD)1. Despite initial demonstration of the benefit of infliximab (IFX) in PCD over 20 years ago2, it remains clear how IFX treatment can be optimised for PCD patients3. In this retrospective observational study, a cohort of PCD patients based at St Mark’s Hospital was reviewed to understand their disease-journeys whilst on treatment with IFX.
Methods
A cohort of 59 patients with PCD on treatment with IFX as of January 2020 were identified from a prospective database of IFX treated patients. Twenty-seven patients were classed as fluctuating IFX levels and underwent disease-journey analysis. Detailed qualitative analysis of individual patients journeys were carried out to correlate IFX levels, where available, to C-Reactive Protein (CRP), Magnetic Resonance Imaging (MRI) and Examinations Under Anaesthetic (EUA). These journeys were then graphed as a timeline for each of these patients.
Results
Four disease-journeys have been selected to exemplify key learning points in the management of PCD.
Graph 1: Improving drainage and reducing inflammatory burden with EUA can help to recover IFX levels and regain disease control. This suggests a well-timed EUA can have a synergistic effect on treatment with IFX.
Graph 2: In a subgroup of patients, optimised medical therapy with IFX alone remains adequate to perianal fistula healing.

Graph 3: Patients may benefit from temporary dose escalations with IFX to recapture response and to improve disease burden.

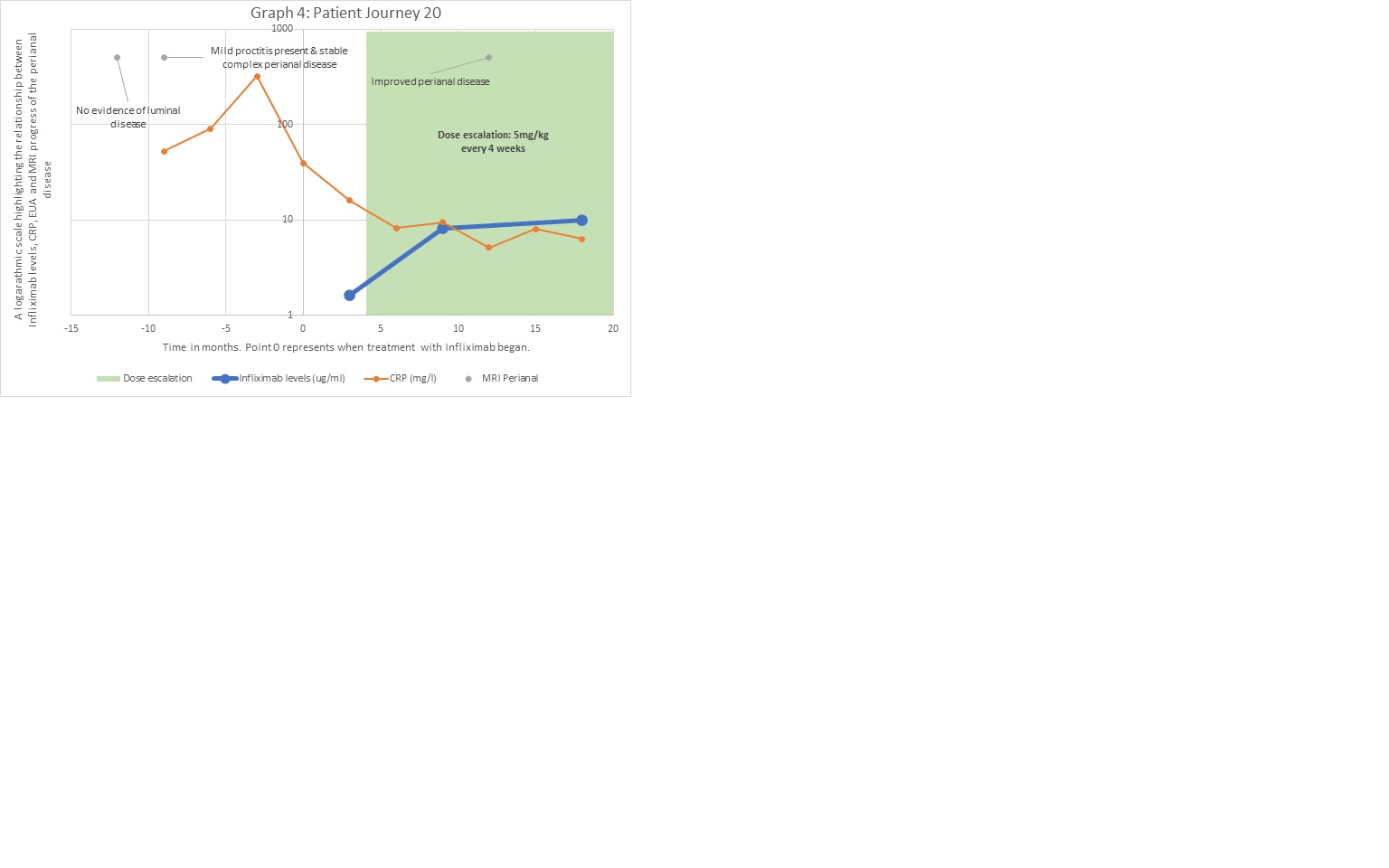
Graph 4: Some patients require longer periods of dose-escalated therapy as seen in this graph & higher IFX levels may be required for radiological healing.
Conclusion
These cases highlight interesting learning points and can help to manage complicated PCD patients. Further work is needed to determine how significant the link is between improvement in IFX levels post-EUA and how this correlates with the overall clinical picture of the patient.
References
1. Sahnan K, Adegbola SO, Fareleira A, Hart A, Warusavitarne J. Medical-surgical Combined Approach in Perianal Fistulizing Crohn's Disease (CD): Doing it Together. Curr Drug Targets. 2019;20(13):1373-1383.
2. Present DH, Rutgeerts P, Targan S, et al. Infliximab for the treatment of fistulas in patients with Crohn's disease. N Engl J Med 1999;340:1398-405.
3. Kotze PG, Shen B, Lightner A, Yamamoto T, Spinelli A, Ghosh S, Panaccione R. Modern management of perianal fistulas in Crohn's disease: future directions. Gut. 2018 Jun;67(6):1181-1194.