
P539 Assessment of age as a risk factor for adverse events in patients from the tofacitinib ulcerative colitis clinical programme
G.R. Lichtenstein1, B. Bressler2, S. Vermeire3, C. Francisconi4, N. Lawendy5, H. Shi5, L. Salese5, D. Judd5, E.V. Loftus Jr6
1Division of Gastroenterology, Perelman School of Medicine at University of Pennsylvania, Philadelphia, PA, USA, 2Division of Gastroenterology, Department of Medicine, University of British Columbia, Vancouver, BC, Canada, 3Department of Gastroenterology, University Hospitals - Leuven, Leuven, Belgium, 4Hospital de Clínicas de Porto Alegre, Porto Alegre, Brazil, Brazil, 5Pfizer Inc., Collegeville, Pennsylvania, USA, 6Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, MN, USA
Background
Tofacitinib is an oral, small-molecule JAK inhibitor for the treatment of UC. Safety and efficacy of tofacitinib were demonstrated in Phase (P)2/3 induction studies, a 52-week, P3 maintenance study, and are being further investigated in an ongoing, open-label, long-term extension (OLE) study.1,2 Here, we provide an updated analysis of age as a risk factor for adverse events (AEs) in the tofacitinib UC clinical programme.3
Methods
Proportions of AEs and serious AEs (SAEs), and incidence rates (IRs; unique patients with events per 100 patient-years) for AEs of special interest (AESIs), were determined for two cohorts: the Maintenance Cohort (patients who received placebo or tofacitinib 5 or 10 mg twice daily [BID] in the maintenance study) and the Overall Cohort (all tofacitinib 5 or 10 mg BID-treated patients in the P2/P3/OLE studies; as of May 2019), stratified by age. Multivariable Cox proportional hazards regression analyses were performed to assess whether older age was associated with increased risk of AESIs in the Overall Cohort.
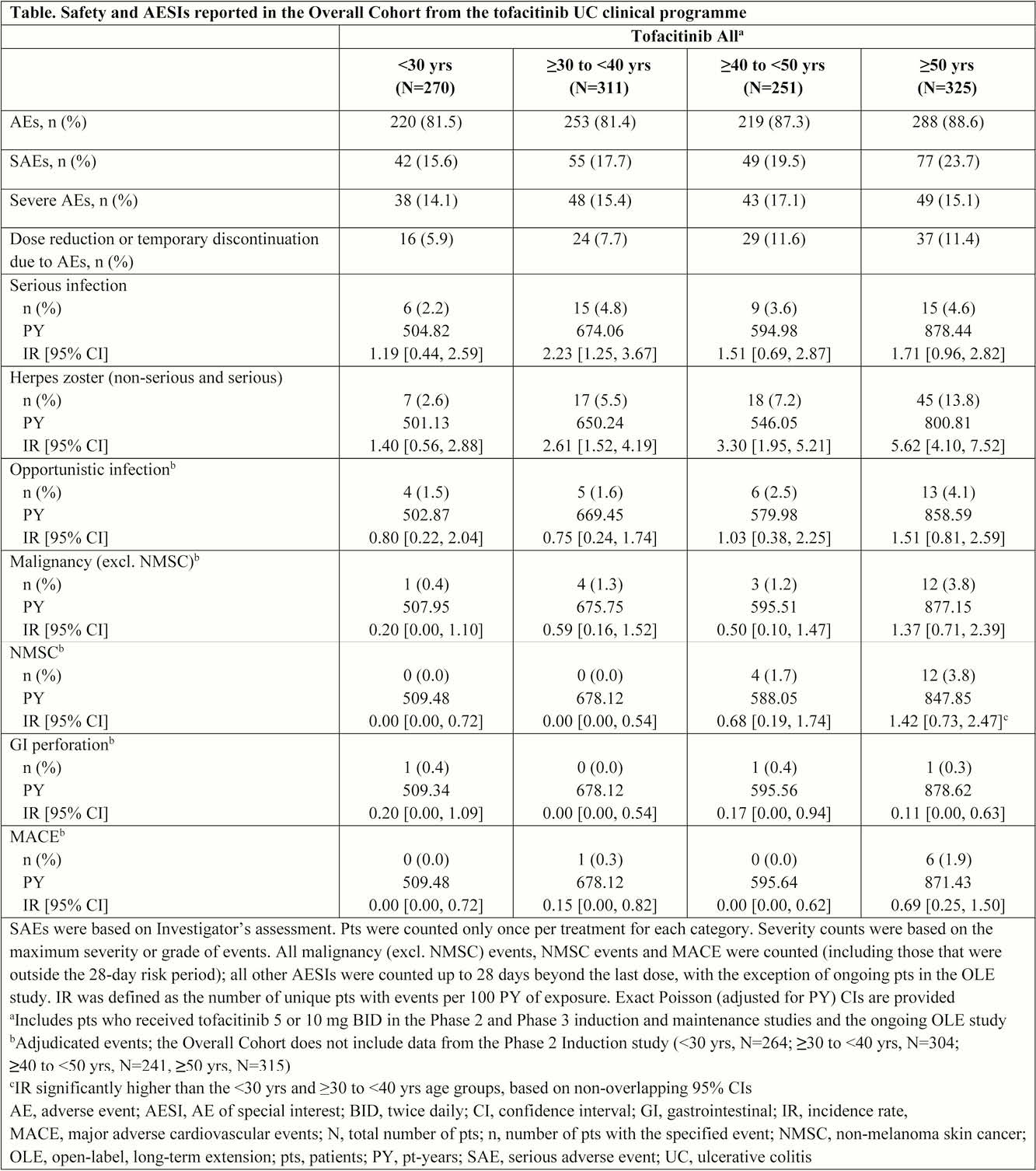
Results
In the Maintenance Cohort, IRs of AEs and SAEs were generally similar between treatment groups, with no age-related trend in the proportions of AEs in tofacitinib-treated patients. AESIs were infrequent in both treatment groups; however, herpes zoster (HZ; non-serious and serious) IRs were numerically higher in the ≥40 to <50 and ≥50 years age groups for patients treated with tofacitinib 10 mg BID vs. placebo and tofacitinib 10 vs. 5 mg BID. In the Overall Cohort, IR of serious infections was generally similar between age groups, while IRs of opportunistic infections (OIs) and HZ (non-serious and serious), malignancy (excl. non-melanoma skin cancer [NMSC]), NMSC and major adverse cardiovascular events increased with increasing age. The IRs of HZ and NMSC were significantly greater in patients ≥50 years compared with patients <30 years, and in patients ≥30 to <40 years for NMSC. In multivariate analyses, older age was identified as a significant predictor of malignancy (excl. NMSC), NMSC and HZ.
Conclusion
In the Overall Cohort, there was a trend for an increase in the rates of OIs, HZ, malignancy (excl. NMSC) and NMSC with increasing age. In multivariate analyses, older age was associated with increased risk of malignancy (excl. NMSC), NMSC and HZ. The results of this analysis are generally consistent with previous studies suggesting older age may be associated with an increased risk of certain AESIs in patients with UC, and in some instances in the general population.4
Sandborn WJ
Lichtenstein GR
Lichtenstein GR
Yawn BP, Gilden D.