
P632 Vedolizumab dose escalation in patients with inflammatory bowel disease experiencing loss of response: A systematic review and meta-analysis of real-world evidence
D. Varghese1, D. Patel2, S. Martin2, M. Luo3, L. Ursos4, R. Lirio5, S. Wang3
1Pharmerit International, Real-World Evidence and Data Analytics, Bethesda, USA, 2Pharmerit International, Strategic Market Access, Bethesda, USA, 3Takeda Pharmaceuticals International, Global Outcomes Research and Epidemiology, Cambridge, USA, 4Takeda Pharmaceuticals USA Inc., US Medical, Deerfield, USA, 5Takeda Development Center Americas, Clinical Science, Cambridge, USA
Background
Moderately to severely active inflammatory bowel disease (IBD), featured as Crohn’s disease (CD) and ulcerative colitis (UC) collectively, is commonly treated with biologic therapies. A proportion of patients experience loss of response (LOR) over time. The approved dose of vedolizumab (VDZ), 300 mg every 8-week (Q8W), is known to be safe and effective in the treatment of UC and CD. In an open-label long-term safety study (GEMINI LTS), patients who experienced LOR during maintenance benefitted from dose escalation to an every 4-week (Q4W) regimen. Clinical response and remission were regained in 41% and 28% respectively in UC patients (N=32) and 47% and 32% respectively in CD patients (N=57) through 52 weeks of escalated dosing. The aim of this study was to conduct a meta-analysis of existing real-world evidences to evaluate the effectiveness of VDZ dose escalation to Q4W in IBD patients experiencing LOR to Q8W dosing.
Methods
A systematic literature review was performed using PubMed and Embase databases for articles and conference abstracts from January 2014 through January 2019 for real-world studies reporting clinical outcomes to VDZ dose-escalation among adult patients with UC or CD. Relevant congresses were also screened for accepted abstracts through June 2019. Summary estimates for the proportion of regained response and remission were synthesised under a random effect model (given considerable heterogeneity as measured by I2 statistic) using the DerSimonian-Laird approach.
Results
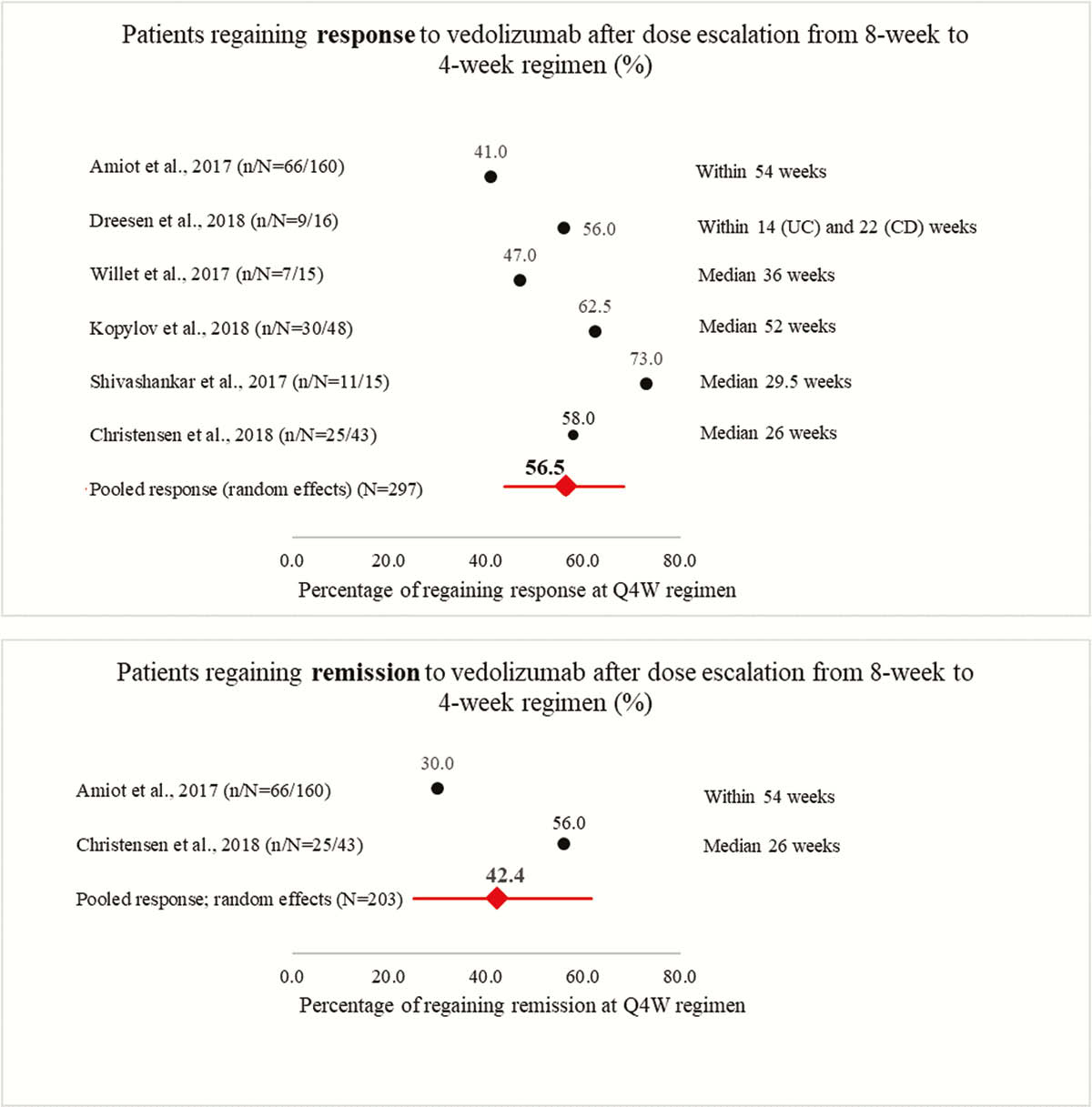
The search yielded a total of 842 citations from the databases and 12 citations from hand searching. Of these, 5 full-text articles and 1 abstract were included in the meta-analysis. The 6 study cohorts included a total of 297 patients with IBD. The random-effects pooled regained response rate from the 6 studies was 56.5% (95% confidence interval [CI], 44.9%–67.5%) within 52 weeks (figure). Subgroup analysis showed a regained response rate of 62.7% (95% CI,52.8%–71.6%) when measured within 30 weeks vs. 50.2% (95% CI, 38.3%–62.2%) when measured after 30 weeks. Of the 6 studies, 2 reported remission rates that were included in the pooled analysis among 203 patients experiencing LOR. The random-effects pooled estimate of recaptured remission was 42.4% (95% CI, 25.1%–61.8%) within 52 weeks.
Conclusion
More than half of IBD patients who experienced LOR during maintenance phase after initial response to VDZ Q8W dosing regained response on the escalated Q4W regimen within 52 weeks. These findings and the data from the open-label clinical trial support the benefits of VDZ dose escalation among patients experiencing LOR to Q8W dosing.