
P771 Increasing prevalence and direct health care cost of inflammatory bowel disease: A population-based evidence from a western Canadian province
J.A. Osei1, J.N. Peña-Sánchez1, S.A. Fowler2, N. Muhajarine1, G. Kaplan3, L.M. Lix4
1University of Saskatchewan, Department of Community Health & Epidemiology- College of Medicine, Saskatoon- SK, Canada, 2University of Saskatchewan, Division of Gastroenterology- College of Medicine, Saskatoon- SK, Canada, 3University of Calgary, Department of Medicine, Calgary, Canada, 4University of Manitoba, Department of Community Health Sciences, Winnipeg, Canada
Background
More than 0.3% of the populations in Europe, North America, and Oceania live with inflammatory bowel disease (IBD). Canada has increasing prevalence trends of IBD with 1% of Canadians estimated to have IBD by 2030. Evidence about IBD prevalence and health care costs over time can contribute to health resources allocation and health care planning. Our study aimed to 1) estimate the prevalence and direct health care costs of IBD in the province of Saskatchewan (SK), Canada, and 2) test if trends in the prevalence and direct health care costs of IBD increased over two decades.
Methods
We conducted a retrospective population-based cohort study using administrative health data of SK between 1999/00 and 2016/17 fiscal years. A validated case definition was used to identify prevalent IBD cases. The costing method adopted by the Canadian Institute for Health Information was used to estimate direct health care costs in 2013/14 Canadian dollars among IBD cases. Generalised linear models (GLMs) with generalised estimating equations were used to test the trends. Negative binomial and gamma distributions were used to, respectively, model prevalence and health care cost trends. Sex and age group were covariates in all models; the Charlson comorbidity index was also included in the cost model. Annual prevalence rates and direct health care cost estimates with their 95% confidence intervals (95%CI) were reported.
Results
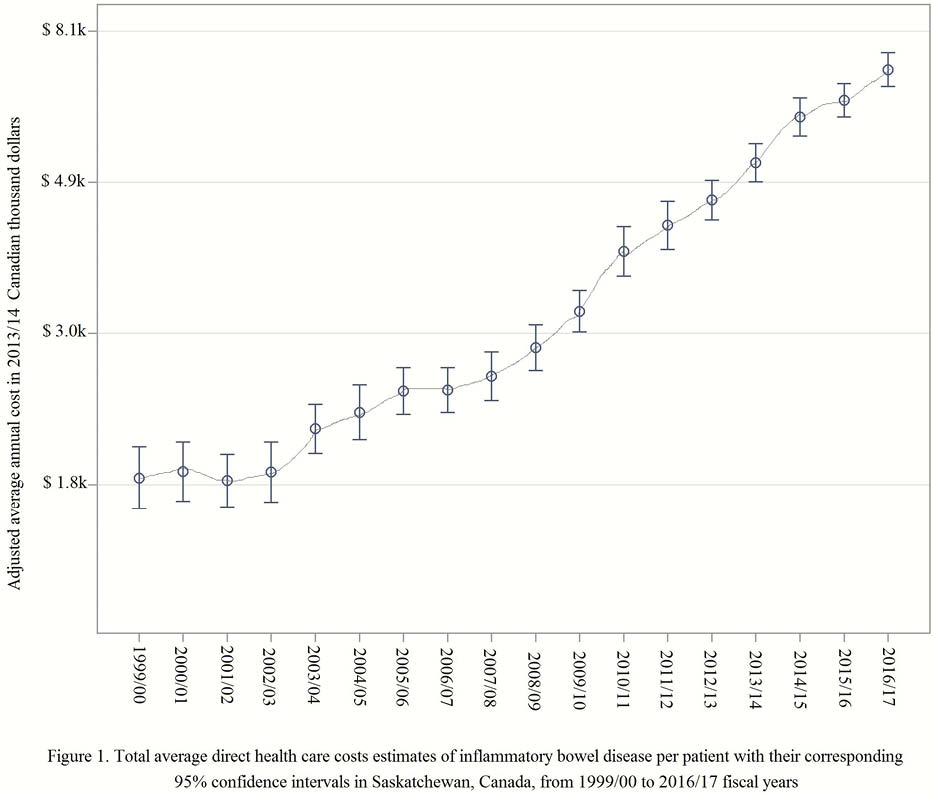
In 2016, there were 6468 (Crohn’s disease: 3663 [56.63%], ulcerative colitis: 2805 [43.37%]) IBD cases ascertained in SK. The number of prevalent cases increased over the analysis period by 56%. The total direct health care costs increased from $7.8 million in 1999 to $50.8 million in 2016. The average annual IBD prevalence increased from 341/100,000 (95%CI 340–341) in 1999 to 664/100,000 (95%CI 663–665) in 2016, a 3.3% (95%CI 2.4–4.3) average annual increase. The total average annual direct health care costs of IBD increased from $1.8 (95%CI $1.6–2.0) thousand per patient in 1999 to $7.1 (95%CI $6.7–7.5) thousand per patient in 2016, an average annual increase of 9.2% (95% CI 8.5–9.8), Figure 1.
Conclusion
In the Canadian province of SK, prevalence and direct health care costs, respectively, tripled and quadrupled over two decades. Our results provide relevant information and analysis on the burden of IBD in SK. These findings are in agreement with previous studies from other provinces. The evidence of constant increasing prevalence and health care cost trends of IBD needs to be recognised by health care decision-makers to promote cost-effective health care policies at provincial and national levels and respond to the needs of patients living with IBD.