
OP18 Surgical prevention of anastomotic recurrence by excluding mesentery in Crohn’s disease: The SuPREMe-CD study
G. Luglio, A. Rispo, N. Imperatore, A. Amendola, F.P. Tropeano, R. Peltrini, F. Castiglione, G.D. De Palma, L. Bucci
Department of Clinical Medicine, Gastroenterology and Surgery, Federico II University of Naples, Naples, Italy
Background
Recently, a new antimesenteric, functional end-to-end, hand-sewn ileocolic anastomosis (Kono-S) has shown a significant reduction in endoscopic recurrence score and surgical recurrence rate in Crohn’s disease (CD).This trial aimed to provide randomised controlled data comparing Kono-S anastomosis and stapled ileocolic side-to-side anastomosis.
Methods
Randomised controlled trial at a tertiary referral institution, enrolling and randomising to undergo either the ‘Kono group’ or the ‘Conventional group’, all CD subjects needing surgery. Primary endpoint: endoscopic recurrence (ER) (Rutgeerts score ≥i2) after 6 months. Secondary endpoints: clinical recurrence (CR) after 12 and 24 months, ER after 18 months and surgical recurrence (SR) after 24 months. Also, short-term outcomes and postoperative complications were recorded. A sample size of 70 patients (35 in each group) was considered necessary to demonstrate a reduction >30% in endoscopic recurrence at 6 months follow-up in the Kono group when assuming a 60% endoscopic recurrence expected rate in the control group.
Results
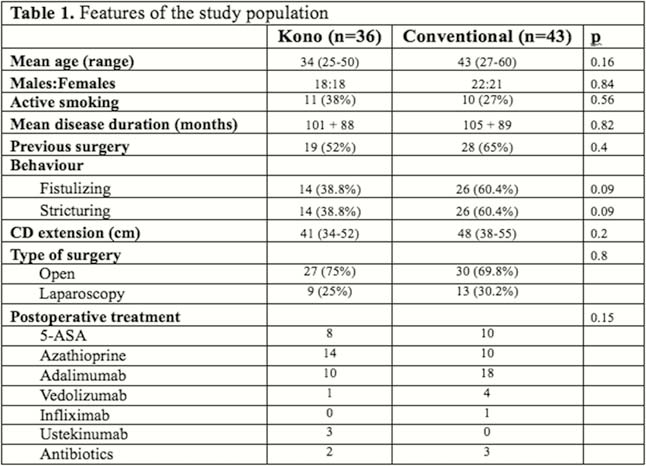
79 CD patients were enrolled and randomised in the Kono group (36) or Conventional group (43) (Table 1). After 6 months, 22.2% in the Kono group and 62.8% in the Conventional group presented an ER (
Conclusion
This is the first RCT comparing Kono-S anastomosis vs. standard anastomosis in CD, which found a significant reduction of postoperative endoscopic recurrence rate by using the novel technique, without concerns about safety. The Kono-S anastomosis could be considered the new recommended surgical technique in CD.
NCT02631967.