
Artificial intelligence – the piece of the puzzle to transform IBD management?
 © Amgen |
This engaging symposium, sponsored by Amgen, took place on July 8, 2021 as part of ECCO’21, and focussed on the role that artificial intelligence (AI) may play in the future management of patients with Inflammatory Bowel Disease (IBD). The symposium was well received and was viewed by over 400 delegates. First, Professor Gionata Fiorino highlighted the importance of early intervention in IBD and how AI approaches might be used to aid early diagnosis. Professor Edouard Louis subsequently discussed the future role that AI may play in the IBD treatment pathway, using examples from other therapy areas. Finally, Professor Walter Reinisch considered how personalised medicine approaches may transform the management of IBD in the future.
Early intervention – fitting the referral and diagnosis pieces together
Gionata Fiorino opened the symposium by highlighting that diagnosis of early-stage IBD, especially Crohn’s Disease (CD) [1], can be challenging due to non-specific symptoms and the lack of a single, non-invasive diagnostic test. As a result, patients with IBD currently experience considerable delays in referral and diagnosis [1, 2]. These delays are a major barrier to early intervention with disease-modifying therapies, particularly in CD, and can lead to disease complications and poor long-term patient outcomes [1, 3].
CD and Ulcerative Colitis (UC) are known to be progressive diseases [3–5]. In eligible patients, early intervention with disease-modifying therapies within ‘a window of opportunity’ can slow progression, prevent irreversible damage and improve long-term patient outcomes [3, 6–8]. In order to facilitate early intervention, approaches to reduce referral times and allow for timely diagnosis of IBD are needed.
The Red Flags Index
Tools such as the Red Flags Index (RFI) for CD have been developed to try and reduce the time to diagnosis and facilitate early intervention; the RFI includes eight items that are independently associated with a diagnosis of CD (Figure 1) [1]. A prospective, observational study performed to validate the RFI revealed a sensitivity of 50% and a specificity of 58% for CD diagnosis [9]. However, combining the RFI with measurement of faecal calprotectin (FCP) significantly improved the diagnostic accuracy, to give a sensitivity of 100% and a specificity of 72% [9]. The results from this study demonstrate the value of combining clinical symptoms and biomarkers to aid in the early referral and diagnosis of CD.
Gionata Fiorino concluded his presentation by noting that AI approaches may further improve the efficiency of referral and diagnostic tools in IBD in the future via:
- Automation of electronic health records (EHR) analysis to identify patients who may fit the criteria for a diagnosis of CD using the RFI
- Identification of items in EHRs associated with a later diagnosis of UC to aid development of a RFI for UC
- Further refinement of the RFI to identify the minimum inputs needed for accurate diagnosis.
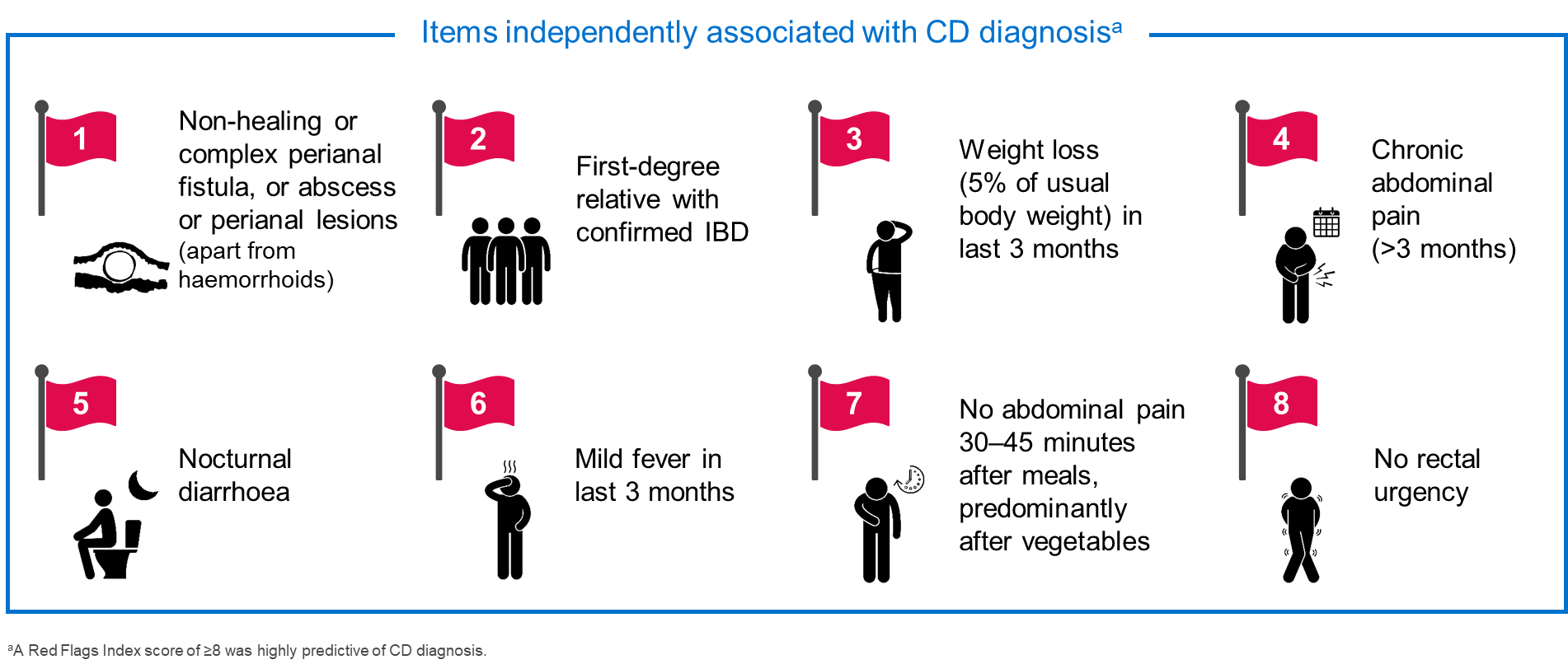
Figure 1: Red Flags Index for the diagnosis of CD [1]
What can AI bring to the patient management puzzle?
Edouard Louis informed the audience that AI is a rapidly evolving field in healthcare, which has the potential to profoundly modify research and patient care [10], and that AI techniques have been used with success in many areas of medicine.
AI approaches are starting to be used in IBD, although use of AI in IBD is not as advanced as in other medical fields (Figure 2). Research has progressed from initial exploratory proof-of-concept studies, through to the development of time-saving AI-based tools, such as algorithms capable of automated image analysis. Algorithms to help guide clinical decisions are beginning to be investigated, but we have still not reached the overall goal of AI, which is to help facilitate a fully personalised treatment approach to improve patient outcomes.
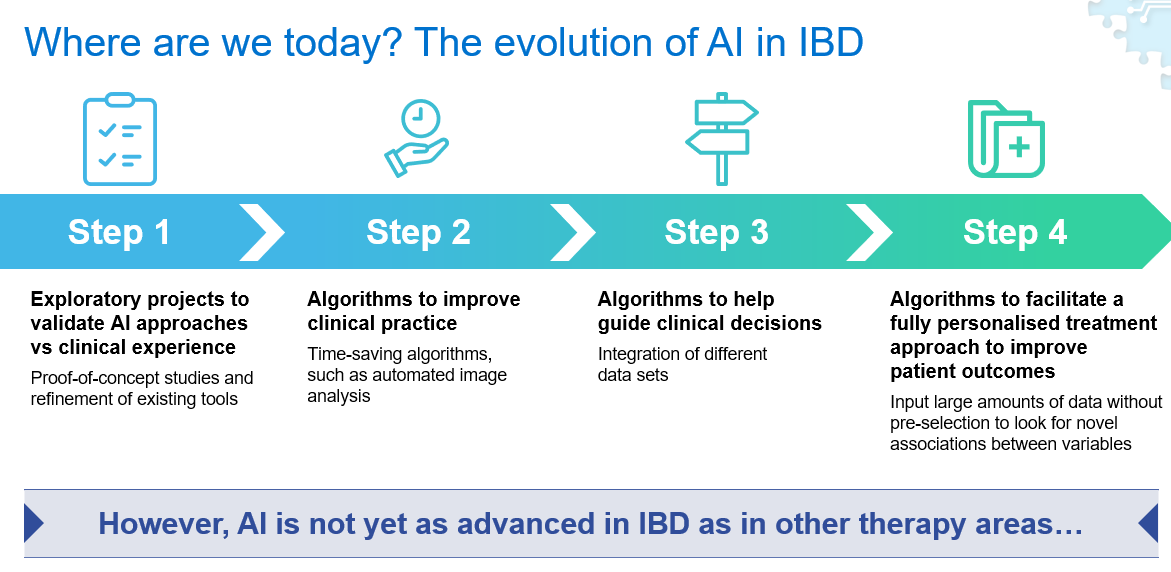
Figure 2: The evolution of AI in IBD
Current and future use of AI in IBD
Tools evaluated in IBD so far have employed AI methodologies to automate image analysis [11–13], and although useful for easing clinician workload, these tools will not revolutionise patient care and only scratch the surface of what AI is capable of.
Edouard Louis went on to discuss what we should be aiming for, as the potential for AI in IBD extends much further than current applications. In the future, AI could be used to analyse vast amounts of unselected data on patient variables and disease outcomes to identify complex patterns and associations that are beyond the scope of the human brain. Such an approach could lead to a new understanding of disease and improved patient management in IBD. For example, AI could be used to integrate a broad range of patient data collected during everyday life, such as blood pressure, sleep cycles and physical activity levels, to predict disease evolution in real time and help to avoid the need for regular invasive testing.
Metabolomics (the analysis of small molecular metabolites in biological samples such as urine, stool, blood and tissue biopsies) is another area where AI is likely to play a role in the future. Metabolomics has already been used to provide insights into IBD pathogenesis [14], and the potential exists for metabolomics to allow enhanced patient stratification for clinical management. Could metabolomic analysis of stool samples coupled with AI techniques, such as machine learning, be used to diagnose IBD or predict relapse in the future?
Edouard Louis also noted that there are many steps in the patient journey where AI could be employed to improve the management of IBD, but the most pressing unmet needs are currently reduction of referral times and prediction of response or relapse to a given therapy. To facilitate a fully personalised treatment approach, AI could be used in these areas to:
- Identify early markers of disease (pre-Red Flags) to aid self-referral to a GP
- Identify variables measured in everyday life that could signal to a GP that a patient should be referred to a gastroenterologist
- Predict treatment response prior to treatment initiation
- Monitor a patient once therapy has commenced for markers that may be predictive of disease relapse.
He concluded by stating that the era of personalised medicine is about to dawn in IBD and AI techniques could allow its full potential to be realised.
The coming-of-age of personalised medicine in the IBD clinic
Walter Reinisch began his presentation by providing some general background on personalised medicine, as well as its use in IBD. Personalised medicine is the tailoring of disease management approaches based on patient-specific factors to help improve patient outcomes. Patient-specific factors related to genetics, epigenetics and the microbiome, as well as clinical and lifestyle factors, are used to tailor disease management in personalised medicine [15]. This approach is of particular value in multiple hit diseases, such as IBD, where patients can be highly heterogeneous due to the complex interplay between genetic and environmental factors that drives the disease pathogenesis [15, 16]. Long-term disease management can be difficult in IBD and personalised medicine is needed to allow selection of the most effective therapy for each individual patient (Figure 3).
In IBD, some aspects of disease management in routine clinical care are already governed in part by personalised medicine, including the use of:
- FCP and C-reactive protein to predict disease course [17, 18] and monitor treatment response [19]
- Therapeutic drug monitoring to guide dose adjustments and optimise outcomes [20].
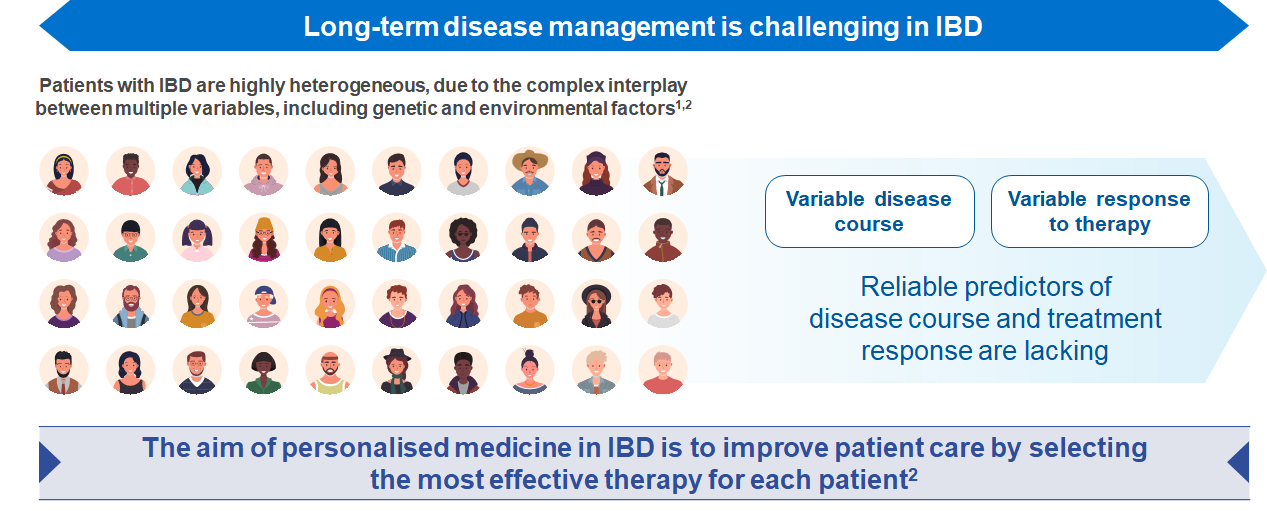
Figure 3: The need for personalised medicine in IBD
Clinical decision support tools
Walter Reinisch went on to describe tools based on commonly collected clinical data that are in development in IBD to help predict response to biologic therapies [21, 22]. A clinical decision support tool was developed to identify factors associated with CD remission following treatment with vedolizumab [21]. Multivariable logistic regression identified variables associated with remission, including no prior bowel surgery, no prior anti-TNF exposure and no prior fistulising disease, as well as baseline albumin and CRP levels. A points system was developed to give a weighting to each variable and a cut-off value of 13 points identified patients in clinical remission, in steroid-free remission or with mucosal healing after vedolizumab with ≥92% sensitivity [21]. Multivariable logistic regression has also been used to predict primary non-response to infliximab in CD. Age at first use of infliximab, body mass index and previous surgery were included in the final predictive model, which demonstrated good accuracy, with an area under the receiver operating characteristic curve (ROC-AUC) of 0.8 (95% CI 0.67–0.93) [22]. In the future, AI techniques could be used to integrate further variables predictive of response, and improve the accuracy and clinical applicability of these tools.
Biomarkers of prognosis and response
Walter Reinisch highlighted that prediction of disease prognosis and response to targeted treatments are key stages in IBD where advances in personalised medicine could help improve patient outcomes.
Genomic risk scores developed using genome-wide single nucleotide polymorphism data could play a future role in predicting disease prognosis. In a study from the International IBD Genetics Consortium, genomic risk score was associated with disease severity in patients with CD; patients with a higher predicted score had clinical characteristics typically associated with a more severe disease course, including requirement for bowel resection (p<0.03), younger age at onset (p<0.005) and ileal disease location (p<0.003) [23]. Analysis of the gut microbiome also offers potential for identification of predictive biomarkers for IBD disease progression. In one study, complex associations were identified between multi-omic components of the gut microbiome and host that may influence disease activity in IBD [24].
Biomarkers of treatment response are also being investigated in IBD. Novel markers of anti-TNF response have been studied in two single-cell analysis studies which revealed that a unique cellular module, consisting of IgG plasma cells, inflammatory mononuclear phagocytes, activated T cells and stromal cells, was significantly associated with anti-TNF response [25] and that inflammatory cell signatures from pre-treatment samples may be associated with future anti-TNF response [26]. While a range of potential biomarkers of response have been identified in IBD, appropriately powered studies are required to validate their use before they can be applied in the clinic.
Challenges surrounding the implementation of personalised medicine in IBD
Several challenges need to be overcome before personalised medicine and AI approaches can implemented in IBD. Research is needed to:
- Further optimise diagnostic criteria in IBD
- Develop definitions of response that are rooted in the biology of the disease, rather than in patient-reported symptoms
- Consolidate opinion on reproducible patient characteristics that can be used to inform personalised medicine approaches, as well as the most appropriate time to assess treatment response.
On a final note, Walter Reinisch summarised how personalised medicine approaches have been implemented successfully in other therapy areas despite similar challenges. In oncology, a companion diagnostic test to predict response to a targeted therapy has been developed in non-small cell lung cancer based on data which identified a clear link between the efficacy of pembrolizumab, a monoclonal antibody that targets the programmed cell death protein, and tumour expression of the PD-1 ligand [27]. Another example is in rheumatoid arthritis, in which machine learning has been used to develop a biomarker panel to predict non-response to anti-TNF [28].
Concluding remarks
AI techniques are emerging in IBD, but further study is needed to allow these tools to reach their full potential in the management of disease. AI-based tools in IBD can be used to ease clinician workload, but AI also has the potential to improve patient outcomes by facilitating early referral and diagnosis, as well predicting prognosis and response to treatment. The era of personalised medicine is only just dawning in IBD. Initial data from clinical decision support tools and novel biomarkers of treatment response need to be validated before they can be used in the clinic to improve patient outcomes. AI techniques may accelerate the search for appropriate personalised medicine tools in the future, but standardisation of various parameters in disease management is needed before the era of personalised medicine in IBD can truly begin.
References
- Danese S, Fiorino G, Mary JY, et al. Development of Red Flags Index for early referral of adults with symptoms and signs suggestive of Crohn's disease: an IOIBD initiative. J Crohns Colitis. 2015;9:601–6.
- Lonnfors S, Vermeire S, Greco M, Hommes D, Bell C, Avedano L. IBD and health-related quality of life -- discovering the true impact. J Crohns Colitis. 2014;8:1281–6.
- Colombel JF, Narula N, Peyrin-Biroulet L. Management strategies to improve outcomes of patients with inflammatory bowel diseases. Gastroenterology. 2017;152:351–61 e355.
- Pariente B, Mary JY, Danese S, et al. Development of the Lemann index to assess digestive tract damage in patients with Crohn's disease. Gastroenterology. 2015;148:52–63 e53.
- Torres J, Billioud V, Sachar DB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis as a progressive disease: the forgotten evidence. Inflamm Bowel Dis. 2012;18:1356–63.
- Danese S, Fiorino G, Peyrin-Biroulet L. Early intervention in Crohn's disease: towards disease modification trials. Gut. 2017;66:2179–87.
- Im JP, Ye BD, Kim YS, Kim JS. Changing treatment paradigms for the management of inflammatory bowel disease. Korean J Intern Med. 2018;33:28–35.
- Amezaga AJ, Van Assche G. Practical approaches to "top-down" therapies for Crohn's disease. Curr Gastroenterol Rep. 2016;18:35.
- Fiorino G, Bonovas S, Gilardi D, et al. Validation of the Red Flags Index for early diagnosis of Crohn's disease: a prospective observational IG-IBD study among general practitioners. J Crohns Colitis. 2020. doi: 10.1093/ecco-jcc/jjaa111. [Online ahead of print].
- Le Berre C, Sandborn WJ, Aridhi S, et al. Application of artificial intelligence to gastroenterology and hepatology. Gastroenterology. 2020;158:76–94 e72.
- Urban G, Tripathi P, Alkayali T, et al. Deep learning localizes and identifies polyps in real time with 96% accuracy in screening colonoscopy. Gastroenterology. 2018;155:1069–78 e1068.
- Seshamani S, Kumar R, Dassopoulos T, Mullin G, Hager G. Augmenting capsule endoscopy diagnosis: a similarity learning approach. Med Image Comput Comput Assist Interv. 2010;13(Pt 2):454–62.
- Ozawa T, Ishihara S, Fujishiro M, et al. Novel computer-assisted diagnosis system for endoscopic disease activity in patients with ulcerative colitis. Gastrointest Endosc. 2019;89:416–21 e411.
- Gallagher K, Catesson A, Griffin JL, Holmes E, Williams HRT. Metabolomic analysis in inflammatory bowel disease: a systematic review. J Crohns Colitis. 2021;15:813–26.
- Seyed Tabib NS, Madgwick M, Sudhakar P, Verstockt B, Korcsmaros T, Vermeire S. Big data in IBD: big progress for clinical practice. Gut. 2020;69:1520–32.
- Graham DB, Xavier RJ. Pathway paradigms revealed from the genetics of inflammatory bowel disease. Nature. 2020;578:527–39.
- Henriksen M, Jahnsen J, Lygren I, et al. C-reactive protein: a predictive factor and marker of inflammation in inflammatory bowel disease. Results from a prospective population-based study. Gut. 2008;57:1518–23.
- Lasson A, Simren M, Stotzer PO, Isaksson S, Ohman L, Strid H. Fecal calprotectin levels predict the clinical course in patients with new onset of ulcerative colitis. Inflamm Bowel Dis. 2013;19:576–81.
- Torres J, Bonovas S, Doherty G, et al. ECCO Guidelines on therapeutics in Crohn's disease: medical treatment. J Crohns Colitis. 2020;14:4–22.
- Colombel JF, Panaccione R, Bossuyt P, et al. Effect of tight control management on Crohn's disease (CALM): a multicentre, randomised, controlled phase 3 trial. Lancet. 2017;390:2779–89.
- Dulai PS, Boland BS, Singh S, et al. Development and validation of a scoring system to predict outcomes of vedolizumab treatment in patients with Crohn's disease. Gastroenterology. 2018;155:687–95 e610.
- Billiet T, Papamichael K, de Bruyn M, et al. A matrix-based model predicts primary response to infliximab in Crohn's disease. J Crohns Colitis. 2015;9:1120–6.
- Chen GB, Lee SH, Montgomery GW, et al. Performance of risk prediction for inflammatory bowel disease based on genotyping platform and genomic risk score method. BMC Med Genet. 2017;18:94.
- Lloyd-Price J, Arze C, Ananthakrishnan AN, et al. Multi-omics of the gut microbial ecosystem in inflammatory bowel diseases. Nature. 2019;569:655–62.
- Martin JC, Chang C, Boschetti G, et al. Single-cell analysis of Crohn's disease lesions identifies a pathogenic cellular module associated with resistance to anti-TNF therapy. Cell. 2019;178:1493–508 e1420.
- Smillie CS, Biton M, Ordovas-Montanes J, et al. Intra- and inter-cellular rewiring of the human colon during ulcerative colitis. Cell. 2019;178:714–30 e722.
- Jorgensen JT. Companion diagnostic assays for PD-1/PD-L1 checkpoint inhibitors in NSCLC. Expert Rev Mol Diagn. 2016;16:131–3.
-
Mellors T, Withers JB, Ameli A, et al. Clinical validation of a blood-based predictive test for stratification of response to tumor necrosis factor inhibitor therapies in rheumatoid arthritis patients. Netw Syst Med. 2020;3.1:91–104.